IMMUNOLOGY REPORT.doc
The Immunology of a Hepatitis B Vaccine Injury in 2009. © Paul A.Taggert.
Complementary Report - available free to the Public in the Public interest.
Report: The Immunology of a Hepatitis B Vaccine Injury in 2009
© Paul A. Taggert
Report: The Immunology of a Hepatitis B Vaccine Injury in 2009. © Paul A.Taggert.
December 2014.
The right of Paul Taggert to be identified as the Author of this work has been asserted in accordance with the Copyright Act of Australia 1968 and its amendments, and international copyright.
NOT FOR SALE
ISBN: 978 – 0 – 9942314 – 3 – 7
For citation, use:
DEDICATION
In memory of: The 53 persons who have died after being injected with Hepatitis B vaccines (HBVs) in the USA. These court- registered deaths up to 04 November 2013, are recorded by the Health Resources and Services Administration
(HRSA)* federal government database. To similar deaths in other countries, we humbly offer the same respect and
acknowledgement. Many thousands more have escaped death, but have not escaped devastating injury of the type
described in this Report.
* www.hrsa.gov/vaccinecompensation
Universal Disclaimer
From good health to wheelie-walker. From sound physiology to chronic disability. Before and after. This text incorporates the Author’s own vaccination record, injury and material facts. As this is the author’s story and research, the author will not accept any responsibility or liability for the actions taken, or results, consequences or outcomes incurred of or to those reading, publishing, printing or utilizing any portion of this written text. The author, provider, publisher and distributor provide no guarantee that the reader of this written text will duplicate any of the results stated herein, if or when undertaking their own clinical or empirical investigations. Any person contemplating whether to vaccinate themselves or their relatives must accept the risk and liability of making their own vaccination choices; accept their own responsibility whether to consult registered or non-registered physicians; and accept the consequences of their own decisions whether to embrace the sciences of policy makers, or the sciences of evidence based medicine. Anyone wishing to utilize any patterns or systems from this text as templates, do so on the condition and understanding that they accept full responsibility and liability for any actions and outcomes resulting from their usage.
Therefore, the contents of this written work is for information purposes and should not be relied upon as the sole source of information relating to the subject matter, or for making medical health decisions. No warranty, either express or implied, is made with respect to the information contained herein. The author, provider, publisher, and
distributor provide no warranty for the content or accuracy, completeness or omission, or usefulness of content of this written work; or for any products, processes or links disclosed herein. Any liability concerning anything done or omitted to be done by any person or entity, from the reading, publishing, printing or utilization of the whole or any part of this written text, is expressly disclaimed.
The author, provider, publisher, and distributor will not assume or accept any legal liability or responsibility for any loss of profit or any other commercial damages resulting from the use of this written text. References herein to any specific
commercial or non commercial product, process, profession, trade name or service, manufacturer, trademark, or otherwise; does not constitute endorsement or disendorsement, favour or discredit, recommendation or rejection of any entities or persons, or their products or services.
The author reserves the right to make alterations, clarifications, modifications, or improvements to this written work; in order to update this work at any time. Any use of this written work signifies your agreement to this Universal Disclaimer.
PREFACE
Pathology has been described as the engine room of Medicine, upon which modern medicine’s foundations were wrought and diagnoses are dependant by the millions. The accumulated scientific evidence contained in this report therefore relies upon this foundational system, driven to it’s obvious conclusion, and which the author relied upon in an Australian compensation claim.
The medico-legal doctors representing the compensation Insurer, failed to include any written evaluation of this prima material evidence in their statements / ‘reports’ to the Insurer, despite the compelling nature of this evidence being at their full disposal. The Insurer and industry Regulator were able to reject the author’s claim entitlement’s based upon the doctor’s omission’s of this evidence. Furthermore, a pre-court Judge ruled it acceptable that the disabled author should have to lie on the floor at his Appeal because of the Judge’s refusal to supply a mobile bed, or reclining padded chair, or to make room for such. The author’s complaints of these vexatious treatments to crime and anti-corruption agencies, fell upon ‘unwilling soles’ who redirected complaints or who denied their veracity. French medico-legal expert and pharmacoepidemiologist Dr. Marc Girard, provided several reports on the author’s injury. Concerning the entrenched culture of denial the author was subjected to, Dr. Girard stated on 9 April 2012: “This is a sheer judicial perversion to discard a medical cause (the vaccine) whose existence in the patient’s environment is clearly documented.” In paraphrasing the remainder of his statement:
‘They, (the Insurer’s doctors) were not content with this alone, but went further by pointing out other trivial causes for his injury, without any credible attempt to trace the least clue of any recent infections or to document those, and thus failed to produce any clinical picture even close to the claimant’s case’. Dr. Girard described their conduct as representing “an impressive illustration of such a perversion”. ‘Utilitas ante Iustitiam’ is a Latin phrase – meaning ‘Expediency before Justice’ – which summarily defines the vexatious treatment the author was subjected to. It is expedient for coordinated and systematic subterfuge to be employed against vaccine injury claims by persons wishing to protect reputation, credibility and careers in medical and government agencies; and professional and commercial interests. These are powerful assets to protect against liability claims. The methods of ‘expediency’ utilised against the author’s compensation claim are typical of their morality. In contrast Cicero stated in 44BC, that it was the function of justice to do no wrong, and that justice must be observed even to the lowest. English writer Quentin Crisp much later ironically declared of modern justice: “The law is simply expediency wearing a long white dress”….. In the case of vaccine injury claims, the ‘law’ and medical bureaucracy share the same bed and wardrobe. It is high time these facts permeated deeper into the public consciousness. As an Australian, the author feels ashamed to have been treated with such expediency and subterfuge, by his fellows in the health and judicial sectors.
ABSTRACT
An autobiographical analysis of independent pathology investigations correlated to observed adverse symptoms of Mr. Paul Taggert (the Author). The analysis taken over a 5 year period, follows a devastating and disabling injury the author acquired after his receipt of two inoculations of the Hepatitis B vaccine in early 2009.
The hypothesis for this analysis is that the Hepatitis B vaccine (HBV) was the sole causal agent for the author’s injury, and that various biological markers in the body would demonstrate an inflammatory-immuno response to the vaccine, resulting in acute and chronic injury to various body systems. The analysis tabulates extensive serum investigations in correlation with radiology findings, clinical examinations, and manufacturer’s declared side-effects. Tabulated data is further demonstrated in line graph illustrations. A Positive Rechallenge event is demonstrated in the data and graphs. The hypothesis also includes the proposition that no pathogens or pre-existing conditions had any causal involvement in the injury sustained. The findings of this investigation show that 15 arbitrary body systems were disrupted soon after receipt of a second inoculation of the same vaccine. Of these, 12 systems remain chronically disrupted after the acute and intermediate phases had passed. The analysis concludes with an 8 point relationship defining a causal link between vaccine and injury. The clinical and empirical evidence therefore fully supports the presented hypothesis.
PATHOLOGY INVESTIGATIONS
- the CLINICAL & EMPIRICAL DATA
SECTIONS:
A): INTRODUCTION 8
B): MATERIALS AND METHODS 10
C): RESULTS OF TESTS 13
D): PROLOGUE and DEFINITIONS 23
E): ANALYSIS AND DISCUSSION 35
F): CONCLUSION 76
APPENDIX 1 78
BIBLIOGRAPHY 80
A): INTRODUCTION:
In early 2009 the Author received two inoculations of the Hepatitis B vaccine (HBV). Within 3 weeks of each injection the author suffered severe flu-like symptoms. The second reaction to the second dose, produced incapacitation so severe that the author was confined to bed for nearly 3 months and was totally dependant upon family for survival. The severity and longevity of the author’s illness after receiving the vaccine warranted extensive pathology investigations including several imaging scans, faecal and urinal analyses, and numerous blood tests. Quite a number of clinical physical examinations were also conducted. The raw data accumulated during this process was tabulated and converted into graphic presentation to provide a visual clarity of the molecular events that had transpired. The content of this report would wrongly be regarded as ‘anecdotal’ or ‘biased’, given that the report incorporates the findings of multiple independent pathology investigations, and is presented in the format and methodology of a standard scientific research work. It is self instructional, compelling and evocative in the evidence of causality it conveys. It sets in place a working standard for identifying and consolidating scientific evidence, in the process of profiling and diagnosing vaccine injuries. This report has been prepared over a 5 year period, mostly while the author was undertaking bed-rest. Its preparation was in the interest of public health and safety.
Author’s Pharmaceutical History:
In the years before 2009 the author’s health was not being managed by a prescribed regimen of pharmaceutical medications, nor was the author involved in the consumption of illegal narcotics or alcoholism. The author practiced a drug-free, alcohol free, physically active lifestyle. Only on occasions did the author resort to a medical practitioner for isolated pharmaceutical assistance.
Author’s Immunisation History:
Exposures to vaccines were very limited. The sum of vaccines received is as follows:
28.1.09 First Hepatitis B vaccine inoculation received. Administrators gave advice that the vaccine was very safe.
19.2.09 22 days later. Severe “viral-like” illness commences. Lasts 6 days. First 2 days of fever. Attended hospital Emergency on 22.2.09.
26.2.09 Due to 1st illness, the author was late in returning for 2nd inoculation. Letter received requesting attendance for 2nd inoculation.
04.3.09 2nd HB inoculation received. Administrator informed of 1st illness.
Administrator dismissed 1st illness as a passing insignificant virus.
25.3.09 21 days later. Severe “viral-like” illness returns. All work ceases.
29.3.09 Attended hospital Emergency again. Confined to bed rest at home for 10 weeks. First 2 weeks of fever. Very ill. Family provided support.
7.6.09 Small energy returns, followed by relapses and returns to bed. Continuing pattern. Chronic symptoms persisting.
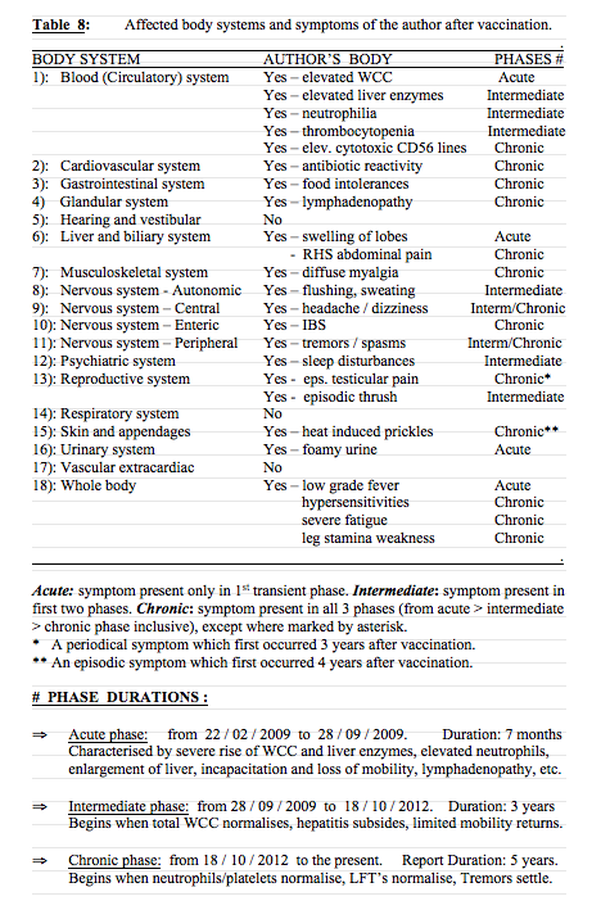
ACUTE SYMPTOMS: ( Duration: for 3 months – following the 2nd injection). Fever – persisting for 2 x weeks. Back aches and tremors. Paralytic stiffening & shakiness of the legs. Severe fatigue. Swollen throbbing lymph glands in neck and armpits. Dry mouth. Sore eyes. Headaches and fuzziness. Poor concentration. Abdominal bloating and churning. Loose frothy and pale stools. Foamy urine.
Irregular sleep. Middle abdominal pain in left (spleen) and right (liver) regions. 1st US scan shows liver inflammation. Elevated LFT’s and WCC. No identifiable diseases.
CHRONIC SYMPTOMS: ( to January 2014: 5 years after the 2nd Inoculation). Mobility Disorder: Legs weakened. Unable to stand on feet for long. Unable to sustain walking as other people regularly and casually do so. Seating or resting required after short use of legs. Short walks of 50-100m require a wheelie-walker with a seat. Walks past 50m can induce leg myalgia and exhaustion flare-up.
Energy Disorder: Severe to exhaustive fatigue, regardless of sleep quality. No stamina. Easily exhausted. Moderate exertion can induce exhaustion flare-up. Daily activity has been significantly slowed and any exertion requires forethought and seating breaks with head support. Intervals of bed rest make up 50% of each day.
Other Systemic Disorder: Daily abdominal pain in RHS liver region at lower rib. Variable body temperatures and abnormal LFT’s persisting for ca. 3.5 years. intolerances to wheaten foods, certain canned foods & oral penicillin drugs. Episodic ‘food poisoning-like’ events. Variable stool formation. Episodic diffuse myalgias. Periodical dizziness. Occasional vertigo. Periodical throbbing or swelling of lymph glands. Occasional excess salivation. Drier skin. Episodic prickles over body induced by heat (‘Prickly heat’). Easily dehydrated. Summer heat intolerance.
B): MATERIALS AND METHODS:
There were at least 12 pathology labs that provided testing of the author’s body fluid donations and imaging scans, including commercial and hospital labs and one university lab. These services were paid for by Australian federal public health system entitlements. The utilization of multiple labs ensured that any unforeseen bias or error could be avoided. The standard practice of not naming service providers in research reports is observed herein, and the identity of the manufacturer who produced the Hepatitis B vaccine is also intentionally omitted from this public report. Where the vaccine proper is directly referred to by the author in this report, it is identified only by its generic name or acronym (HBV), and not by it’s registered trade name. The type and results of all blood tests are collated in Tables 1, 2, & 3. Tabulating these results has provided clarification of the progressive changes the author’s body underwent.
Also included in the pathology investigations are the results of tests undertaken some seven weeks before the vaccination event, which were conducted in relation to a repetitive strain injury the author had been suffering from (restricted to the forearms only), due to many years of rigorous cleaning work. The pre-vaccination pathology data serves as a reliable and timely ‘control’ against which subsequent tests may be compared.
Chemical Components of a typical recombinant Hepatitis B Vaccine:
Pathogen component: The surface protein of Hepatitis B virus, derived from genetically engineered yeast cells, or Chinese hamster ovaries. The hollow virus represents the genetically modified pathogen, achieved via recombinant technology.
Adjuvant component: The immune activator or stimulator, such as: Aluminium hydroxide (a metallic salt of aluminium); or Amorphous aluminium hydroxyphosphate sulphate; or Potassium aluminium sulphate.
Other components: Other ingredients usually include from the following: amino acids, dextrose, mineral salts, soy peptone, sodium phosphate, salt, sodium acid phosphate, polysorbate 20, water, formaldehyde and thiomersal (an ethyl of mercury). These function as buffers, stabilizers, preservatives or fill.
Culturing: Exposure to Bovine (cattle) derived materials, or yeast protein, used for growth medium. The bovine materials may contain animal proteins and microbial pathogens. PIL The Product Information Leaflet. The PIL may contain 5,000 words compressed onto two sides of a folded slip of paper, equal to about 1 x A4 page. Legibility may require a magnifier.
Side – Effects of Hepatitis B Vaccines (HBV’s):
SYNDROMES: (As variously disclosed by drug manufacturer’s & GP’s):
Chronic Fatigue Syndrome (CFS), Bell’s Palsy, Guillaine-barre` Syndrome (GBS), Lymphadenopathy, Multiple Sclerosis (MS) and parallel states, Neuropathy states, Rheumatoid states, Systemic Lupus Erythematosis (SLE). (Other sources add Autism, Chronic Inflammatory Demyelinating Polyneuropathy (CIDP), Coeliac Disease and parallel states, Devic’s Syndrome (DS), Diabetes mellitus, Irritable Bowel Syndrome (IBS), Macrophagic myofasciitis (MMF), and Stevens-Johnson Syndrome (SJS).
ADVERSE SYMPTOMS: (These may be delayed weeks or months):
An extensive array of symptoms are listed in PIL’s including: fatigue, weakness, myelitis, seizure, radiculopathy, migraine, myalgia, hypesthesia, encephalitis, arthritis, flushing, sweating, fever, chills, malaise, anaphylaxis, convulsions, syncope, low blood pressure, paraesthesia – numbness or tingling in extremities, dizziness, vertigo, leg paralysis, optic neuritis – blurred vision, drooping eyelid, meningitis, neck stiffness, vomiting diarrhoea, abdominal pain, anorexia, hepatitis, abnormal liver enzymes, tinnitus, erythemas, ecchymosis, angioderma, thrombocytopenia, disturbed sleep, bronchial spasms, pharyngitis, cough, sore throat, runny nose, dysuria - difficulty passing urine, vasculitis, swollen and throbbing lymph glands, nausea, back pain, aches and pains, loss of appetite, etc.
FREQUENCY OF INJURY:
The incidence of systemic HBV side effects (meaning chronic genetic damage) from clinical trials has been acknowledged by pharmacos to be about 8% - 10%. Australian Therapeutic Goods Administration received 10 adverse reports per week over a 3.5 year period (between January 2009 and June 2012). Some of these reports relate to combination vaccines, where identifying the offending component is difficult. VAERS holds some 60,000 adverse reports relating to HBV’s.
Pathology Testing Materials, Equipment and Methodology:
Many samples of the author’s serum, urine and faecal fluids were collected for testing. On one occasion, 8 vials of blood were extracted for analysis. There are more than 20 blood collections listed in this work. A variety of tests were performed from each collection, as is usual practice. US, CT and MRI machines were also utilised. Standard testing equipment in commercial serology laboratories include autoclaves, blood gas analysers, centrifuses, cell counters, colorimeters, computers, distillation apparatus, glucometers, microscopes, haemocytometers, haemometers, hot air ovens, incubators, petri cultures, pipettes, ph meters, refrigeration units, scales, esr-settling stands, thermo cyclers, various stainless utensils, vortex shakers, etc. Table 1 below outlines the method of body fluid profiling utilized to acquire diagnostic data, to confirm or dismiss the proposed hypothesis of this investigation.
Table 1: Profiling methodology of body fluid investigations of Paul Taggert, utilized to define a causal link and exclusion diagnoses.
GENERAL NON - PATHOGENIC TESTS :
Celiac Disease
Cholesterol
Co-enzyme Q 10
Creatine Kinase
*Full Blood Counts.
Hormonal: Aldosterone
Cortisol
DHEAS
Glucose
Testosterone
Thyroid
Liver Function Tests:
Minerals : Ferritin, Zinc
Magnesium
Prostrate (PSA)
Vitamins B 12, D3, Folate
.
AUTO IMMUNE DISORDERS :
Auto Antibodies Master
Anti-neutrophil Cytoplasmic A/b
Anti – nuclear Antibody
CSF Immunoglobulin G
Cytokines
DNA Antibodies
Extractable Nuclear AG
Neuronal (Myelin) Antibodies
NK Cells and KI Receptors
T-Cell & B-Cell lineages
Rheumatoid Factor
MOSQUITO PATHOGENS :
Barmah Forest Virus
Ross River Virus
HEPATITIS PATHOGENS : Hepatitis A, B, C, Viruses
STD PATHOGENS : Chlamydia
Gonorrhoea
HIV .
MISCELLANEOUS PATHOGENS : Cytomegalovirus (CMV)
Epstein Barr Virus (EBV)
Faecal Analyses
Q Fever
Pneumonia
Toxoplasmosis
C Reactive Protein
Erythrocyte Sediment’n Rate
Urine Micro Culture .
RESULTS OF TESTS:
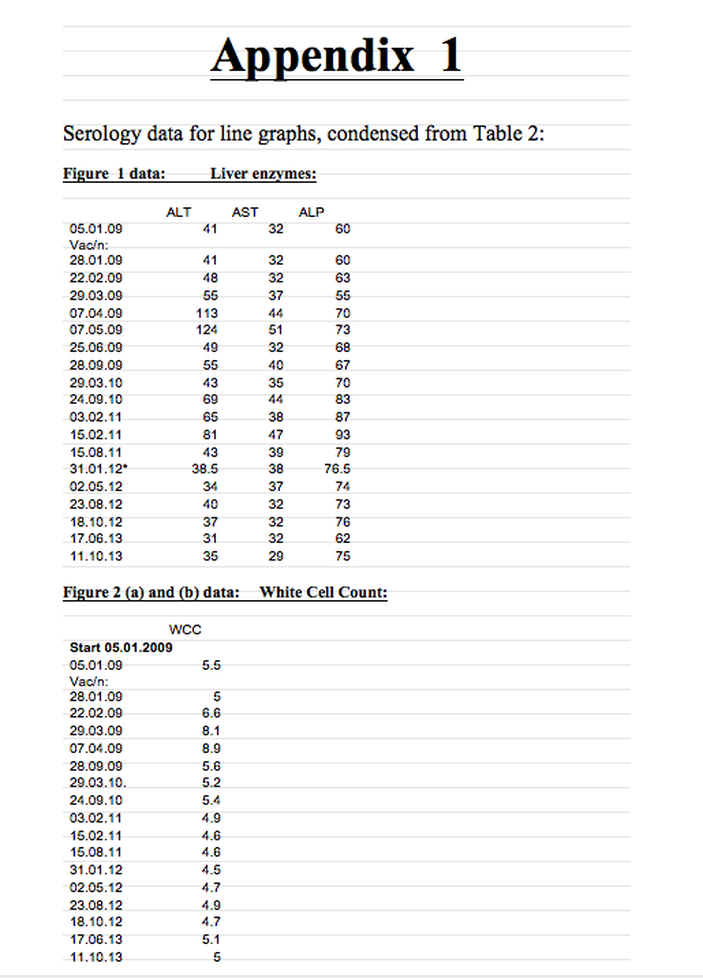
The pathology results in the following pages of this section, are chronologically ordered and listed within Tables 2 & 3:
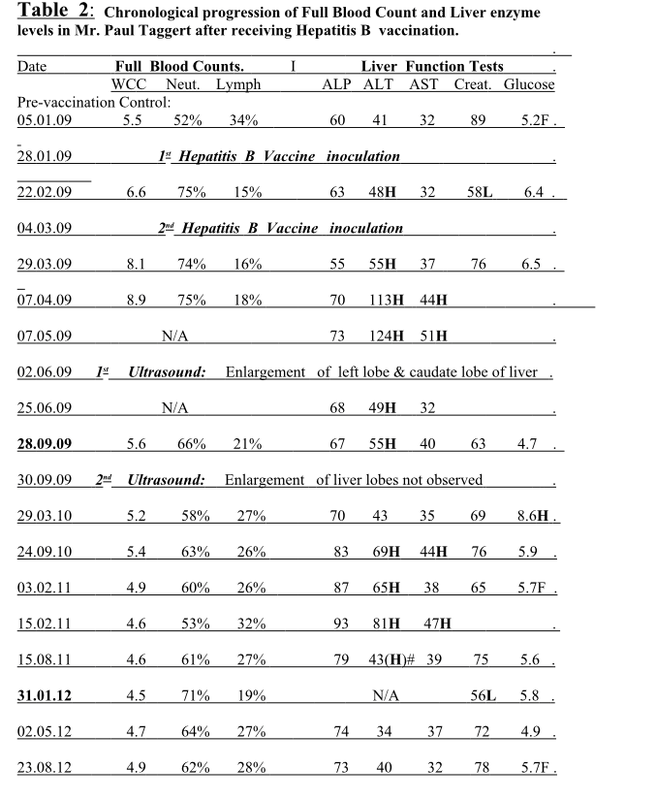
Table 2: Chronological progression of Full Blood Count and Liver enzyme levels in Mr. Paul Taggert after receiving Hepatitis B vaccination.
SEE PAGE 14 for Table 2 ……………………………………….>/
Table 2 - Key: Range Limits:
WCC: White Cell Count 4.0 – 11.0
Neut: Neutrophils % of WBC
Lymph: Lymphocytes % of WBC
ALP: Alkaline phosphatase (liver enzyme) 30 - 115
ALT: Alanine transaminase (liver enzyme) 0 - 45
AST: Aspartate transaminase (liver enzyme) 0 - 41
Creat: Creatinine (kidney function) 60 - 140
Gluco: Glucose (Sugar balance) 3.0 - 7.8
F: Fasting
H: Higher than normal. L: Lower than normal
# Range limits vary slightly between commercial service providers.
FBC: Full blood count
LFT: Liver Function Test
* First test result to roughly correspond with the Control results of 05.01.2009.
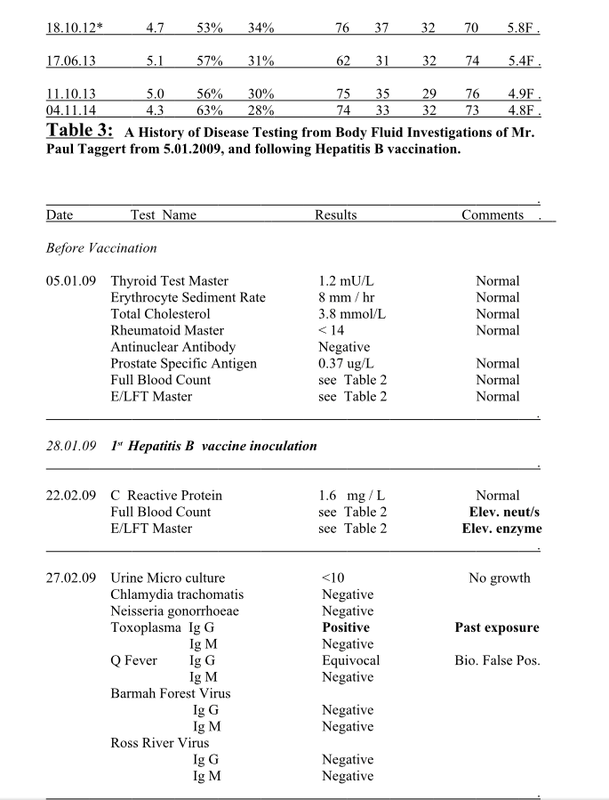
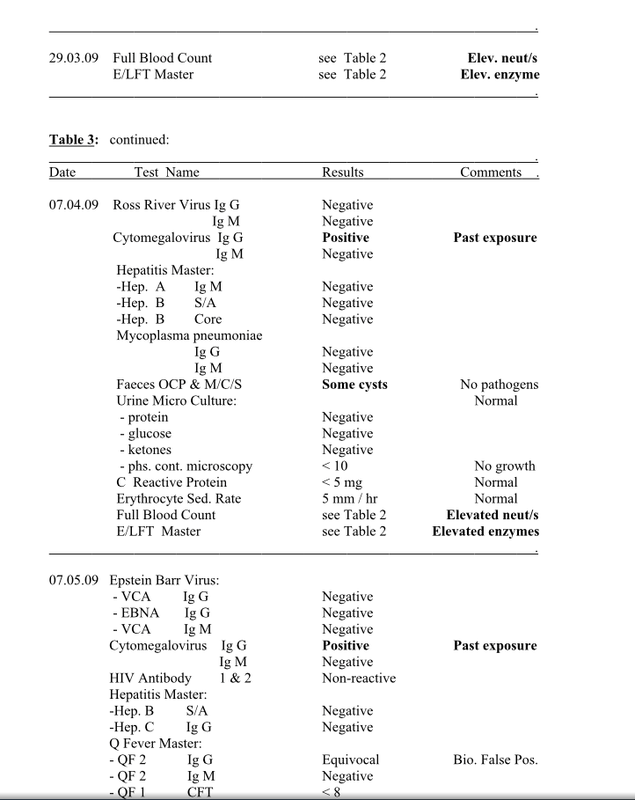
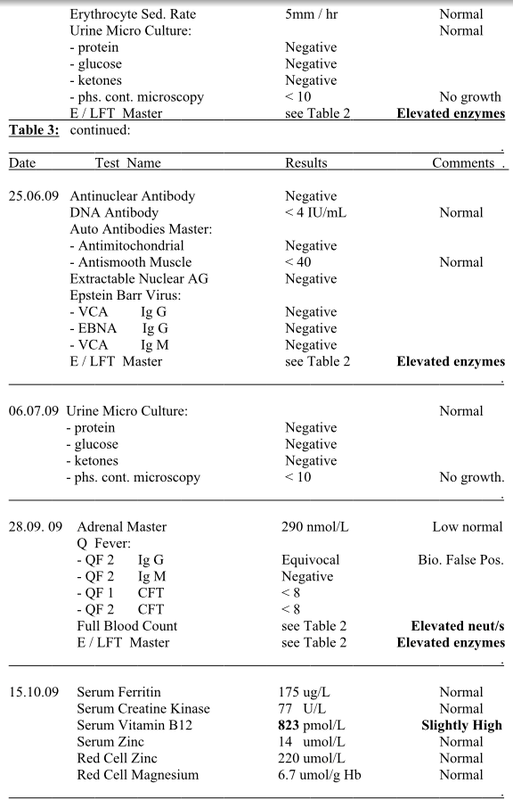
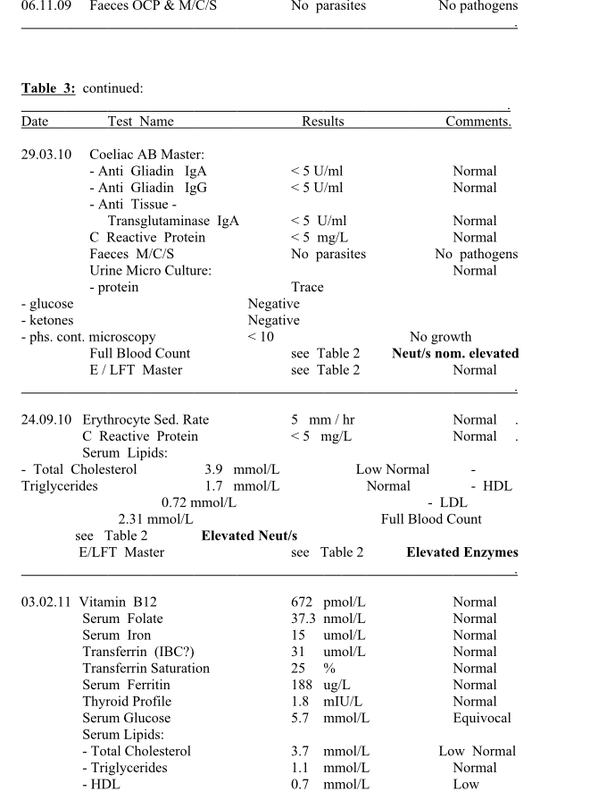
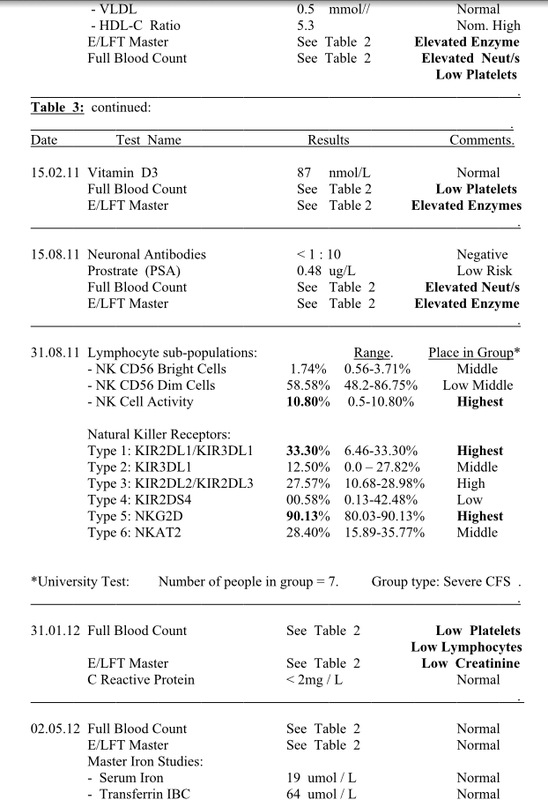
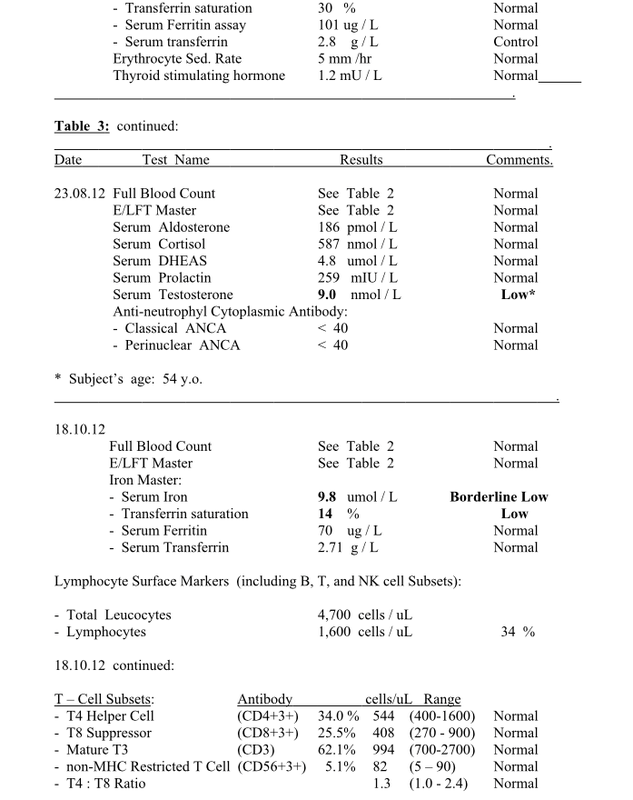
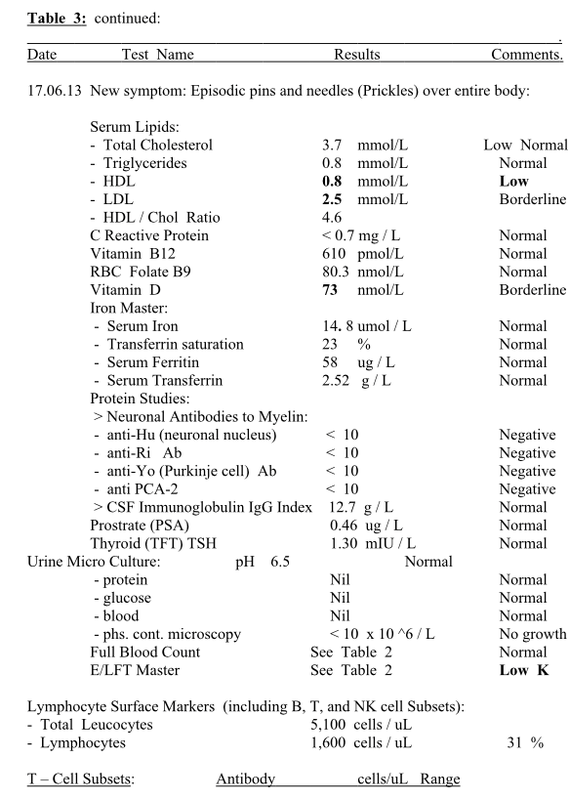
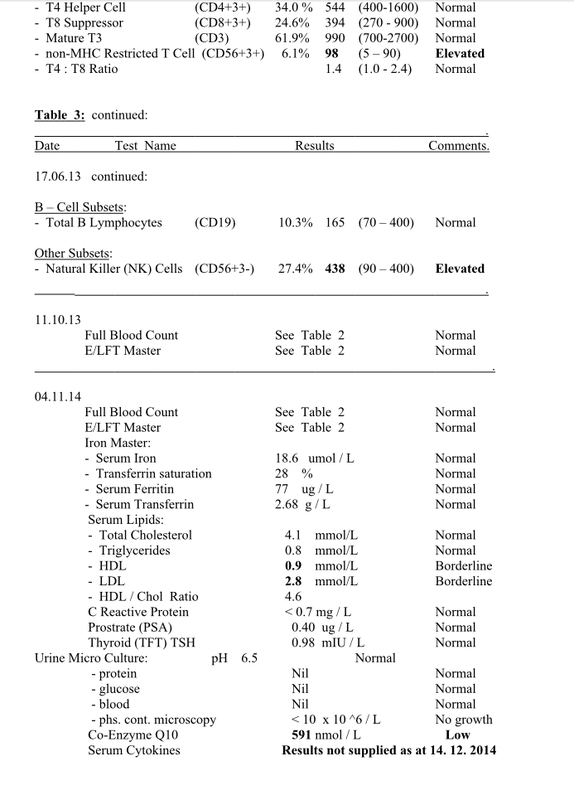
Table 3: A History of Disease Testing from Body Fluid Investigations of Mr.
Paul Taggert from 5.1.2009, and following Hepatitis B vaccination.
14Complementary Report - available free to the Public in the Public interest.
SEE PAGES 15 – 22 for Table 3 ...………………………………>/
Results and comments are provided alongside each test name. This Table provides data for an exclusion diagnosis, or pre-existing conditions or pathogenic infections.
The Immunology of a Hepatitis B Vaccine Injury in 2009. © Paul A.Taggert.
Complementary Report - available free to the Public in the Public interest.
Report: The Immunology of a Hepatitis B Vaccine Injury in 2009
© Paul A. Taggert
Report: The Immunology of a Hepatitis B Vaccine Injury in 2009. © Paul A.Taggert.
December 2014.
The right of Paul Taggert to be identified as the Author of this work has been asserted in accordance with the Copyright Act of Australia 1968 and its amendments, and international copyright.
NOT FOR SALE
ISBN: 978 – 0 – 9942314 – 3 – 7
For citation, use:
DEDICATION
In memory of: The 53 persons who have died after being injected with Hepatitis B vaccines (HBVs) in the USA. These court- registered deaths up to 04 November 2013, are recorded by the Health Resources and Services Administration
(HRSA)* federal government database. To similar deaths in other countries, we humbly offer the same respect and
acknowledgement. Many thousands more have escaped death, but have not escaped devastating injury of the type
described in this Report.
* www.hrsa.gov/vaccinecompensation
Universal Disclaimer
From good health to wheelie-walker. From sound physiology to chronic disability. Before and after. This text incorporates the Author’s own vaccination record, injury and material facts. As this is the author’s story and research, the author will not accept any responsibility or liability for the actions taken, or results, consequences or outcomes incurred of or to those reading, publishing, printing or utilizing any portion of this written text. The author, provider, publisher and distributor provide no guarantee that the reader of this written text will duplicate any of the results stated herein, if or when undertaking their own clinical or empirical investigations. Any person contemplating whether to vaccinate themselves or their relatives must accept the risk and liability of making their own vaccination choices; accept their own responsibility whether to consult registered or non-registered physicians; and accept the consequences of their own decisions whether to embrace the sciences of policy makers, or the sciences of evidence based medicine. Anyone wishing to utilize any patterns or systems from this text as templates, do so on the condition and understanding that they accept full responsibility and liability for any actions and outcomes resulting from their usage.
Therefore, the contents of this written work is for information purposes and should not be relied upon as the sole source of information relating to the subject matter, or for making medical health decisions. No warranty, either express or implied, is made with respect to the information contained herein. The author, provider, publisher, and
distributor provide no warranty for the content or accuracy, completeness or omission, or usefulness of content of this written work; or for any products, processes or links disclosed herein. Any liability concerning anything done or omitted to be done by any person or entity, from the reading, publishing, printing or utilization of the whole or any part of this written text, is expressly disclaimed.
The author, provider, publisher, and distributor will not assume or accept any legal liability or responsibility for any loss of profit or any other commercial damages resulting from the use of this written text. References herein to any specific
commercial or non commercial product, process, profession, trade name or service, manufacturer, trademark, or otherwise; does not constitute endorsement or disendorsement, favour or discredit, recommendation or rejection of any entities or persons, or their products or services.
The author reserves the right to make alterations, clarifications, modifications, or improvements to this written work; in order to update this work at any time. Any use of this written work signifies your agreement to this Universal Disclaimer.
PREFACE
Pathology has been described as the engine room of Medicine, upon which modern medicine’s foundations were wrought and diagnoses are dependant by the millions. The accumulated scientific evidence contained in this report therefore relies upon this foundational system, driven to it’s obvious conclusion, and which the author relied upon in an Australian compensation claim.
The medico-legal doctors representing the compensation Insurer, failed to include any written evaluation of this prima material evidence in their statements / ‘reports’ to the Insurer, despite the compelling nature of this evidence being at their full disposal. The Insurer and industry Regulator were able to reject the author’s claim entitlement’s based upon the doctor’s omission’s of this evidence. Furthermore, a pre-court Judge ruled it acceptable that the disabled author should have to lie on the floor at his Appeal because of the Judge’s refusal to supply a mobile bed, or reclining padded chair, or to make room for such. The author’s complaints of these vexatious treatments to crime and anti-corruption agencies, fell upon ‘unwilling soles’ who redirected complaints or who denied their veracity. French medico-legal expert and pharmacoepidemiologist Dr. Marc Girard, provided several reports on the author’s injury. Concerning the entrenched culture of denial the author was subjected to, Dr. Girard stated on 9 April 2012: “This is a sheer judicial perversion to discard a medical cause (the vaccine) whose existence in the patient’s environment is clearly documented.” In paraphrasing the remainder of his statement:
‘They, (the Insurer’s doctors) were not content with this alone, but went further by pointing out other trivial causes for his injury, without any credible attempt to trace the least clue of any recent infections or to document those, and thus failed to produce any clinical picture even close to the claimant’s case’. Dr. Girard described their conduct as representing “an impressive illustration of such a perversion”. ‘Utilitas ante Iustitiam’ is a Latin phrase – meaning ‘Expediency before Justice’ – which summarily defines the vexatious treatment the author was subjected to. It is expedient for coordinated and systematic subterfuge to be employed against vaccine injury claims by persons wishing to protect reputation, credibility and careers in medical and government agencies; and professional and commercial interests. These are powerful assets to protect against liability claims. The methods of ‘expediency’ utilised against the author’s compensation claim are typical of their morality. In contrast Cicero stated in 44BC, that it was the function of justice to do no wrong, and that justice must be observed even to the lowest. English writer Quentin Crisp much later ironically declared of modern justice: “The law is simply expediency wearing a long white dress”….. In the case of vaccine injury claims, the ‘law’ and medical bureaucracy share the same bed and wardrobe. It is high time these facts permeated deeper into the public consciousness. As an Australian, the author feels ashamed to have been treated with such expediency and subterfuge, by his fellows in the health and judicial sectors.
ABSTRACT
An autobiographical analysis of independent pathology investigations correlated to observed adverse symptoms of Mr. Paul Taggert (the Author). The analysis taken over a 5 year period, follows a devastating and disabling injury the author acquired after his receipt of two inoculations of the Hepatitis B vaccine in early 2009.
The hypothesis for this analysis is that the Hepatitis B vaccine (HBV) was the sole causal agent for the author’s injury, and that various biological markers in the body would demonstrate an inflammatory-immuno response to the vaccine, resulting in acute and chronic injury to various body systems. The analysis tabulates extensive serum investigations in correlation with radiology findings, clinical examinations, and manufacturer’s declared side-effects. Tabulated data is further demonstrated in line graph illustrations. A Positive Rechallenge event is demonstrated in the data and graphs. The hypothesis also includes the proposition that no pathogens or pre-existing conditions had any causal involvement in the injury sustained. The findings of this investigation show that 15 arbitrary body systems were disrupted soon after receipt of a second inoculation of the same vaccine. Of these, 12 systems remain chronically disrupted after the acute and intermediate phases had passed. The analysis concludes with an 8 point relationship defining a causal link between vaccine and injury. The clinical and empirical evidence therefore fully supports the presented hypothesis.
PATHOLOGY INVESTIGATIONS
- the CLINICAL & EMPIRICAL DATA
SECTIONS:
A): INTRODUCTION 8
B): MATERIALS AND METHODS 10
C): RESULTS OF TESTS 13
D): PROLOGUE and DEFINITIONS 23
E): ANALYSIS AND DISCUSSION 35
F): CONCLUSION 76
APPENDIX 1 78
BIBLIOGRAPHY 80
A): INTRODUCTION:
In early 2009 the Author received two inoculations of the Hepatitis B vaccine (HBV). Within 3 weeks of each injection the author suffered severe flu-like symptoms. The second reaction to the second dose, produced incapacitation so severe that the author was confined to bed for nearly 3 months and was totally dependant upon family for survival. The severity and longevity of the author’s illness after receiving the vaccine warranted extensive pathology investigations including several imaging scans, faecal and urinal analyses, and numerous blood tests. Quite a number of clinical physical examinations were also conducted. The raw data accumulated during this process was tabulated and converted into graphic presentation to provide a visual clarity of the molecular events that had transpired. The content of this report would wrongly be regarded as ‘anecdotal’ or ‘biased’, given that the report incorporates the findings of multiple independent pathology investigations, and is presented in the format and methodology of a standard scientific research work. It is self instructional, compelling and evocative in the evidence of causality it conveys. It sets in place a working standard for identifying and consolidating scientific evidence, in the process of profiling and diagnosing vaccine injuries. This report has been prepared over a 5 year period, mostly while the author was undertaking bed-rest. Its preparation was in the interest of public health and safety.
Author’s Pharmaceutical History:
In the years before 2009 the author’s health was not being managed by a prescribed regimen of pharmaceutical medications, nor was the author involved in the consumption of illegal narcotics or alcoholism. The author practiced a drug-free, alcohol free, physically active lifestyle. Only on occasions did the author resort to a medical practitioner for isolated pharmaceutical assistance.
Author’s Immunisation History:
Exposures to vaccines were very limited. The sum of vaccines received is as follows:
- circa 1966: oral vaccine x 1 - 10ml. cup of pink syrup, taken in primary school years. Syrup probably contained Sabin Polio vaccine.
- Tetanus vaccines x 3, at 15 year intervals in adult life.
- No reactions detected at the time of those vaccinations.
- 28 / 01 / 2009: 1st inoculation with Hepatitis B vaccine.
- Delayed response injury (DRI) occurred 3 weeks after inoculation.
- 04 / 03 / 2009: 2nd Hepatitis B inoculation received.
- Delayed response injury reoccurs, again 3 weeks after inoculation.
- Same constellation of symptoms as 1st DRI. (A Positive Rechallenge event).
- 2nd DRI more severe. 3 months bed confinement. Chronic disability acquired.
28.1.09 First Hepatitis B vaccine inoculation received. Administrators gave advice that the vaccine was very safe.
19.2.09 22 days later. Severe “viral-like” illness commences. Lasts 6 days. First 2 days of fever. Attended hospital Emergency on 22.2.09.
26.2.09 Due to 1st illness, the author was late in returning for 2nd inoculation. Letter received requesting attendance for 2nd inoculation.
04.3.09 2nd HB inoculation received. Administrator informed of 1st illness.
Administrator dismissed 1st illness as a passing insignificant virus.
25.3.09 21 days later. Severe “viral-like” illness returns. All work ceases.
29.3.09 Attended hospital Emergency again. Confined to bed rest at home for 10 weeks. First 2 weeks of fever. Very ill. Family provided support.
7.6.09 Small energy returns, followed by relapses and returns to bed. Continuing pattern. Chronic symptoms persisting.
ACUTE SYMPTOMS: ( Duration: for 3 months – following the 2nd injection). Fever – persisting for 2 x weeks. Back aches and tremors. Paralytic stiffening & shakiness of the legs. Severe fatigue. Swollen throbbing lymph glands in neck and armpits. Dry mouth. Sore eyes. Headaches and fuzziness. Poor concentration. Abdominal bloating and churning. Loose frothy and pale stools. Foamy urine.
Irregular sleep. Middle abdominal pain in left (spleen) and right (liver) regions. 1st US scan shows liver inflammation. Elevated LFT’s and WCC. No identifiable diseases.
CHRONIC SYMPTOMS: ( to January 2014: 5 years after the 2nd Inoculation). Mobility Disorder: Legs weakened. Unable to stand on feet for long. Unable to sustain walking as other people regularly and casually do so. Seating or resting required after short use of legs. Short walks of 50-100m require a wheelie-walker with a seat. Walks past 50m can induce leg myalgia and exhaustion flare-up.
Energy Disorder: Severe to exhaustive fatigue, regardless of sleep quality. No stamina. Easily exhausted. Moderate exertion can induce exhaustion flare-up. Daily activity has been significantly slowed and any exertion requires forethought and seating breaks with head support. Intervals of bed rest make up 50% of each day.
Other Systemic Disorder: Daily abdominal pain in RHS liver region at lower rib. Variable body temperatures and abnormal LFT’s persisting for ca. 3.5 years. intolerances to wheaten foods, certain canned foods & oral penicillin drugs. Episodic ‘food poisoning-like’ events. Variable stool formation. Episodic diffuse myalgias. Periodical dizziness. Occasional vertigo. Periodical throbbing or swelling of lymph glands. Occasional excess salivation. Drier skin. Episodic prickles over body induced by heat (‘Prickly heat’). Easily dehydrated. Summer heat intolerance.
B): MATERIALS AND METHODS:
There were at least 12 pathology labs that provided testing of the author’s body fluid donations and imaging scans, including commercial and hospital labs and one university lab. These services were paid for by Australian federal public health system entitlements. The utilization of multiple labs ensured that any unforeseen bias or error could be avoided. The standard practice of not naming service providers in research reports is observed herein, and the identity of the manufacturer who produced the Hepatitis B vaccine is also intentionally omitted from this public report. Where the vaccine proper is directly referred to by the author in this report, it is identified only by its generic name or acronym (HBV), and not by it’s registered trade name. The type and results of all blood tests are collated in Tables 1, 2, & 3. Tabulating these results has provided clarification of the progressive changes the author’s body underwent.
Also included in the pathology investigations are the results of tests undertaken some seven weeks before the vaccination event, which were conducted in relation to a repetitive strain injury the author had been suffering from (restricted to the forearms only), due to many years of rigorous cleaning work. The pre-vaccination pathology data serves as a reliable and timely ‘control’ against which subsequent tests may be compared.
Chemical Components of a typical recombinant Hepatitis B Vaccine:
Pathogen component: The surface protein of Hepatitis B virus, derived from genetically engineered yeast cells, or Chinese hamster ovaries. The hollow virus represents the genetically modified pathogen, achieved via recombinant technology.
Adjuvant component: The immune activator or stimulator, such as: Aluminium hydroxide (a metallic salt of aluminium); or Amorphous aluminium hydroxyphosphate sulphate; or Potassium aluminium sulphate.
Other components: Other ingredients usually include from the following: amino acids, dextrose, mineral salts, soy peptone, sodium phosphate, salt, sodium acid phosphate, polysorbate 20, water, formaldehyde and thiomersal (an ethyl of mercury). These function as buffers, stabilizers, preservatives or fill.
Culturing: Exposure to Bovine (cattle) derived materials, or yeast protein, used for growth medium. The bovine materials may contain animal proteins and microbial pathogens. PIL The Product Information Leaflet. The PIL may contain 5,000 words compressed onto two sides of a folded slip of paper, equal to about 1 x A4 page. Legibility may require a magnifier.
Side – Effects of Hepatitis B Vaccines (HBV’s):
SYNDROMES: (As variously disclosed by drug manufacturer’s & GP’s):
Chronic Fatigue Syndrome (CFS), Bell’s Palsy, Guillaine-barre` Syndrome (GBS), Lymphadenopathy, Multiple Sclerosis (MS) and parallel states, Neuropathy states, Rheumatoid states, Systemic Lupus Erythematosis (SLE). (Other sources add Autism, Chronic Inflammatory Demyelinating Polyneuropathy (CIDP), Coeliac Disease and parallel states, Devic’s Syndrome (DS), Diabetes mellitus, Irritable Bowel Syndrome (IBS), Macrophagic myofasciitis (MMF), and Stevens-Johnson Syndrome (SJS).
ADVERSE SYMPTOMS: (These may be delayed weeks or months):
An extensive array of symptoms are listed in PIL’s including: fatigue, weakness, myelitis, seizure, radiculopathy, migraine, myalgia, hypesthesia, encephalitis, arthritis, flushing, sweating, fever, chills, malaise, anaphylaxis, convulsions, syncope, low blood pressure, paraesthesia – numbness or tingling in extremities, dizziness, vertigo, leg paralysis, optic neuritis – blurred vision, drooping eyelid, meningitis, neck stiffness, vomiting diarrhoea, abdominal pain, anorexia, hepatitis, abnormal liver enzymes, tinnitus, erythemas, ecchymosis, angioderma, thrombocytopenia, disturbed sleep, bronchial spasms, pharyngitis, cough, sore throat, runny nose, dysuria - difficulty passing urine, vasculitis, swollen and throbbing lymph glands, nausea, back pain, aches and pains, loss of appetite, etc.
FREQUENCY OF INJURY:
The incidence of systemic HBV side effects (meaning chronic genetic damage) from clinical trials has been acknowledged by pharmacos to be about 8% - 10%. Australian Therapeutic Goods Administration received 10 adverse reports per week over a 3.5 year period (between January 2009 and June 2012). Some of these reports relate to combination vaccines, where identifying the offending component is difficult. VAERS holds some 60,000 adverse reports relating to HBV’s.
Pathology Testing Materials, Equipment and Methodology:
Many samples of the author’s serum, urine and faecal fluids were collected for testing. On one occasion, 8 vials of blood were extracted for analysis. There are more than 20 blood collections listed in this work. A variety of tests were performed from each collection, as is usual practice. US, CT and MRI machines were also utilised. Standard testing equipment in commercial serology laboratories include autoclaves, blood gas analysers, centrifuses, cell counters, colorimeters, computers, distillation apparatus, glucometers, microscopes, haemocytometers, haemometers, hot air ovens, incubators, petri cultures, pipettes, ph meters, refrigeration units, scales, esr-settling stands, thermo cyclers, various stainless utensils, vortex shakers, etc. Table 1 below outlines the method of body fluid profiling utilized to acquire diagnostic data, to confirm or dismiss the proposed hypothesis of this investigation.
Table 1: Profiling methodology of body fluid investigations of Paul Taggert, utilized to define a causal link and exclusion diagnoses.
GENERAL NON - PATHOGENIC TESTS :
Celiac Disease
Cholesterol
Co-enzyme Q 10
Creatine Kinase
*Full Blood Counts.
Hormonal: Aldosterone
Cortisol
DHEAS
Glucose
Testosterone
Thyroid
Liver Function Tests:
Minerals : Ferritin, Zinc
Magnesium
Prostrate (PSA)
Vitamins B 12, D3, Folate
.
AUTO IMMUNE DISORDERS :
Auto Antibodies Master
Anti-neutrophil Cytoplasmic A/b
Anti – nuclear Antibody
CSF Immunoglobulin G
Cytokines
DNA Antibodies
Extractable Nuclear AG
Neuronal (Myelin) Antibodies
NK Cells and KI Receptors
T-Cell & B-Cell lineages
Rheumatoid Factor
MOSQUITO PATHOGENS :
Barmah Forest Virus
Ross River Virus
HEPATITIS PATHOGENS : Hepatitis A, B, C, Viruses
STD PATHOGENS : Chlamydia
Gonorrhoea
HIV .
MISCELLANEOUS PATHOGENS : Cytomegalovirus (CMV)
Epstein Barr Virus (EBV)
Faecal Analyses
Q Fever
Pneumonia
Toxoplasmosis
C Reactive Protein
Erythrocyte Sediment’n Rate
Urine Micro Culture .
RESULTS OF TESTS:
The pathology results in the following pages of this section, are chronologically ordered and listed within Tables 2 & 3:
Table 2: Chronological progression of Full Blood Count and Liver enzyme levels in Mr. Paul Taggert after receiving Hepatitis B vaccination.
SEE PAGE 14 for Table 2 ……………………………………….>/
Table 2 - Key: Range Limits:
WCC: White Cell Count 4.0 – 11.0
Neut: Neutrophils % of WBC
Lymph: Lymphocytes % of WBC
ALP: Alkaline phosphatase (liver enzyme) 30 - 115
ALT: Alanine transaminase (liver enzyme) 0 - 45
AST: Aspartate transaminase (liver enzyme) 0 - 41
Creat: Creatinine (kidney function) 60 - 140
Gluco: Glucose (Sugar balance) 3.0 - 7.8
F: Fasting
H: Higher than normal. L: Lower than normal
# Range limits vary slightly between commercial service providers.
FBC: Full blood count
LFT: Liver Function Test
* First test result to roughly correspond with the Control results of 05.01.2009.
Table 3: A History of Disease Testing from Body Fluid Investigations of Mr.
Paul Taggert from 5.1.2009, and following Hepatitis B vaccination.
14Complementary Report - available free to the Public in the Public interest.
SEE PAGES 15 – 22 for Table 3 ...………………………………>/
Results and comments are provided alongside each test name. This Table provides data for an exclusion diagnosis, or pre-existing conditions or pathogenic infections.

Other Subsets:
Natural killer (NK) Cells (CD 56+3-) 27.1% 434 (90-400) elevated
Natural killer (NK) Cells (CD 56+3-) 27.1% 434 (90-400) elevated
D: PROLOGUE to Discussion:
Genetic Sensitivity and Immunologist’s Dirty Little Secret.
In understanding the author’s immune-based injury, it is necessary to briefly review the human genome and the practices of the field of Immunotherapy / pharmacy that lead to the development of anti-cancer drugs and vaccine drugs.
The human genome is a complex mix of biochemistry under-written by a genetic constitution fixed to each genotype. Like all animals with intrinsic cross-breeding safeguards, human genotypes are highly specific and cannot interbreed with other close relatives within the primates. Likewise, the human genome is very unforgiving of genetic intervention and consequently harbours many bio-rejection factors within our makeup. These factors cause side-effects and hypersensitivity reactions to drugs in people, and can result in permanent genetic damage to some recipients.
Understanding the hypersensitivity of the human genome is made easier when some perspective is applied. That perspective readily comes when comparing humans to our closest primate relative - the Chimpanzee. Humans share 98% of the same DNA codes with chimps, yet amazingly, that remaining 2% of different DNA produces two entirely different species of vastly differing capabilities and potential. (We don’t see chimps building rockets to the moon, baking bread in ovens, or writing Shakespearean plays, now do we!). That 2% of difference points to a universal law of genetics - Small differences in system protocols produces big changes in appearance, function and capability. In simpler terms – small changes produces big results.
What then would a 2% change (or less) to your own genetic constitution, do to your system balance, function, and stability? This is what happens when infections occur. Foreign pathogens with their own genomic protocols enter our genetic environment, and temporarily affect our systems making us sick. Many of us successfully deal with those invasions according to our ecological heritage and species diversity. Likewise, vaccines - with their own genetically modified pathogens and inorganic ingredients - invade our genetic/blood environment, bypassing our protective barriers and causing change. Furthermore, that artificial invasion is instituted outside our ecological development, and can disturb our system protocols so profoundly that permanent changes arise. The law then applies: Small changes produces big malfunctions (and sometimes death).
Just as a small electronic virus disturbs the program format that underwrites your computer’s main system, so also a genetically modified vaccine can disturb the genetic program that underwrites and controls many human body systems. The ideology relied upon by authoritarian health agencies that ‘the benefits of vaccines far outweigh the risks (of injury)’ is an ideology that currently is not supported by credible science, especially when weighed against the laws of genetics. The laws of genetics point us to the inevitable conclusion that the advertised benefits are not credible, and that the risks are significant. One drug manufacturer has acknowledged in their own product information leaflet that the risk of acquiring systemic (genetic) injury from their HBV cocktail is 8%.
Genetic Sensitivity and Immunologist’s Dirty Little Secret.
In understanding the author’s immune-based injury, it is necessary to briefly review the human genome and the practices of the field of Immunotherapy / pharmacy that lead to the development of anti-cancer drugs and vaccine drugs.
The human genome is a complex mix of biochemistry under-written by a genetic constitution fixed to each genotype. Like all animals with intrinsic cross-breeding safeguards, human genotypes are highly specific and cannot interbreed with other close relatives within the primates. Likewise, the human genome is very unforgiving of genetic intervention and consequently harbours many bio-rejection factors within our makeup. These factors cause side-effects and hypersensitivity reactions to drugs in people, and can result in permanent genetic damage to some recipients.
Understanding the hypersensitivity of the human genome is made easier when some perspective is applied. That perspective readily comes when comparing humans to our closest primate relative - the Chimpanzee. Humans share 98% of the same DNA codes with chimps, yet amazingly, that remaining 2% of different DNA produces two entirely different species of vastly differing capabilities and potential. (We don’t see chimps building rockets to the moon, baking bread in ovens, or writing Shakespearean plays, now do we!). That 2% of difference points to a universal law of genetics - Small differences in system protocols produces big changes in appearance, function and capability. In simpler terms – small changes produces big results.
What then would a 2% change (or less) to your own genetic constitution, do to your system balance, function, and stability? This is what happens when infections occur. Foreign pathogens with their own genomic protocols enter our genetic environment, and temporarily affect our systems making us sick. Many of us successfully deal with those invasions according to our ecological heritage and species diversity. Likewise, vaccines - with their own genetically modified pathogens and inorganic ingredients - invade our genetic/blood environment, bypassing our protective barriers and causing change. Furthermore, that artificial invasion is instituted outside our ecological development, and can disturb our system protocols so profoundly that permanent changes arise. The law then applies: Small changes produces big malfunctions (and sometimes death).
Just as a small electronic virus disturbs the program format that underwrites your computer’s main system, so also a genetically modified vaccine can disturb the genetic program that underwrites and controls many human body systems. The ideology relied upon by authoritarian health agencies that ‘the benefits of vaccines far outweigh the risks (of injury)’ is an ideology that currently is not supported by credible science, especially when weighed against the laws of genetics. The laws of genetics point us to the inevitable conclusion that the advertised benefits are not credible, and that the risks are significant. One drug manufacturer has acknowledged in their own product information leaflet that the risk of acquiring systemic (genetic) injury from their HBV cocktail is 8%.
This figure, derived from post-marketing surveillance, is likely to be conservative given the reluctance of doctors to report vaccine reactions to officials.
The field of Immunotherapy has been growing steadily over recent decades, promising lucrative careers for research Immunologists and Geneticists, and allied personnel. Unfortunately, scientific breakthroughs in this field have not been commensurately generous. The literature reveals that the field has been characterised by much hit and miss experimentation, as researchers utilize various approaches of lymphocyte activation in order to develop rescue mechanisms for combating various diseases, including vaccine counter-measures against biological agents.
Contrary to the claims of vaccine campaigners, advances in immunology have been very slow and highly dependant upon experimental biology. The division of the immune system for example, into the Innate and Adaptive faculties remained poorly understood right up to the 1990’s. True and deep understanding of immunity up to that time had become bogged down by the habitual practice by many researchers of ‘lacing’ experiments with adjuvants (such as oxides of aluminium) in order to bully B and T cells into obedience. This practice prevailed because most vaccine developers knew nothing of the Innate immune system. They wrongly believed that B and T lymphocytes were the only cells to drive the immune response, and that adjuvants were invariably necessary to stimulate this system to work faster and more effectively. This blunt approach became known in some quarters as “Immunologist’s dirty little secret” – a phrase used by renowned American immunologist (#) Professor Charles A. Janeway Jr., who was concerned about drug developer’s dependency upon crude adjuvants for propagating desired results. Janeway voiced his concerns in his address to the Cold Spring Harbor Symposium in the USA (Janeway 1989, 1-13).
Adjuvanted ‘lacing’ in vaccine development meant that much of the vaccine industry up to the 1990’s had thus been propagated upon a brutalized method of experimental immunology, while simultaneously being deficient in a thorough and sympathetic understanding of protective immunity and genetic vulnerability. Even more concerning, is that much of that erroneous mindset was imposed upon gullible populations during vaccination campaigns, and delivered as: ‘We are highly trained doctors and researchers, authorities in health, we know what we are doing – this is for your own good, trust us’. Such smug arrogance led to the shocking increase in MS in France following the HBV campaigns of 1994-8, and many other vaccine injuries worldwide.
Disturbed by the unscrupulous behavior of vaccine developers, Charles Janeway began to investigate why adjuvants were even necessary for protective immunity. Could not the immune system do without these? Before 1990, there were precious few facts concerning the Innate immunity, with early thoughts originating from predecessors such as Macfarlane Burnet in 1967 and Niels Jerne in 1976. Between 1990 and 2000 however, Janeway together with immunologist wife Kim Bottomly and other researchers such as Yang Lui and Ruslan Medzhitov, identified many facts supporting the theory that a separate faculty of the immune system existed, which oversaw the Adaptive immunity.
Thus, within a 10 year period Janeway and collegues managed to re-write the immunology model, by demonstrating that exposure to antigens alone was insufficient to activate the Adaptive immunity. They showed that any induction of the Adaptive immunity was subject to a higher immune authority of more ancient origin, where under the control of genetically engrained protocol, molecular signaling must first be released by this higher authority before adaptive cells could be activated. This primordial faculty – the Innate immunity – operated using evolutionarily conserved pattern recognition receptors (PRR’s) rather than antibodies, and in hindsight simply explains why a person can be very sick but show little lymphocyte activation on their serology printouts – its because the Innate immunity is already hard at work, and it decides when and how much lymphocyte activation it requires to defeat an infection, without causing self harm to the host.
There was the difference – self modulating and benevolent immune engagement, as opposed to brute synthetic activation derived from crude adjuvants. Immunologist’s dirty little secret - of ‘lacing’ vaccines with adjuvants - was now exposed. Janeway’s new model showed there were three signals necessary before T lymphocytes could be released into the fight. Thus, antigenic invasion triggers the following signals:
Signal 1: Activation of PRR’s on macophages and dendritic cells, followed by recognition and binding to antigens. Neutrophils assist in destroying antigens by acting independently.
Signal 2: Upregulation of co-stimulatory molecules and cytokines (triggered by the macrophages and dendritic cells), to prepare for B lymphocyte activation if required.
Signal 3: Elaboration of pro-inflammatory cytokines to form and activate B cells, which then guide new and existing T lymphocytes into elite specialised killing forces.
Thus, the orthodox immunology establishment got a big lesson in how the primordial immune system functioned, and that tampering with those delicate protocols was unwise. Although Janeway’s discoveries have led to some new vaccine recipes which utilize PRR’s rather than adjuvants, amazingly, the brutal practice of adjuvanted immunology still prevails today together with the devastating injuries they incite. The whistle-blowing of Janeway and later, Gherardi (2003), and others appear to have been ignored by the pharmaceutical engine and health bureaucracies alike, because we find in the immunology literature numerous studies which persist in lymphocyte stimulation with the view to cornering some chemical device to be sold as an anti-disease vaccine. Thus, in the decade after Janeway’s passing, the reader still can witness questionable practices such as:
Immunophenotyping, antigen independent stimulation, cytokine driven changes, altered expression, polyclonal cell activation, stimulation triggering, cytokine stimulation, induced cytotoxicity, activated phenotype, selective expansion, coordinated induction, insertion cloning, high dose therapy, tumour blockading, genetic engineering, sustained secretion, modulation and modification; recombinant technology, genetically modified antigen, haptenated antigen, delivery of antigen-encoding genes, virus-derived vectors, and so on.
The field of Immunotherapy has been growing steadily over recent decades, promising lucrative careers for research Immunologists and Geneticists, and allied personnel. Unfortunately, scientific breakthroughs in this field have not been commensurately generous. The literature reveals that the field has been characterised by much hit and miss experimentation, as researchers utilize various approaches of lymphocyte activation in order to develop rescue mechanisms for combating various diseases, including vaccine counter-measures against biological agents.
Contrary to the claims of vaccine campaigners, advances in immunology have been very slow and highly dependant upon experimental biology. The division of the immune system for example, into the Innate and Adaptive faculties remained poorly understood right up to the 1990’s. True and deep understanding of immunity up to that time had become bogged down by the habitual practice by many researchers of ‘lacing’ experiments with adjuvants (such as oxides of aluminium) in order to bully B and T cells into obedience. This practice prevailed because most vaccine developers knew nothing of the Innate immune system. They wrongly believed that B and T lymphocytes were the only cells to drive the immune response, and that adjuvants were invariably necessary to stimulate this system to work faster and more effectively. This blunt approach became known in some quarters as “Immunologist’s dirty little secret” – a phrase used by renowned American immunologist (#) Professor Charles A. Janeway Jr., who was concerned about drug developer’s dependency upon crude adjuvants for propagating desired results. Janeway voiced his concerns in his address to the Cold Spring Harbor Symposium in the USA (Janeway 1989, 1-13).
Adjuvanted ‘lacing’ in vaccine development meant that much of the vaccine industry up to the 1990’s had thus been propagated upon a brutalized method of experimental immunology, while simultaneously being deficient in a thorough and sympathetic understanding of protective immunity and genetic vulnerability. Even more concerning, is that much of that erroneous mindset was imposed upon gullible populations during vaccination campaigns, and delivered as: ‘We are highly trained doctors and researchers, authorities in health, we know what we are doing – this is for your own good, trust us’. Such smug arrogance led to the shocking increase in MS in France following the HBV campaigns of 1994-8, and many other vaccine injuries worldwide.
Disturbed by the unscrupulous behavior of vaccine developers, Charles Janeway began to investigate why adjuvants were even necessary for protective immunity. Could not the immune system do without these? Before 1990, there were precious few facts concerning the Innate immunity, with early thoughts originating from predecessors such as Macfarlane Burnet in 1967 and Niels Jerne in 1976. Between 1990 and 2000 however, Janeway together with immunologist wife Kim Bottomly and other researchers such as Yang Lui and Ruslan Medzhitov, identified many facts supporting the theory that a separate faculty of the immune system existed, which oversaw the Adaptive immunity.
Thus, within a 10 year period Janeway and collegues managed to re-write the immunology model, by demonstrating that exposure to antigens alone was insufficient to activate the Adaptive immunity. They showed that any induction of the Adaptive immunity was subject to a higher immune authority of more ancient origin, where under the control of genetically engrained protocol, molecular signaling must first be released by this higher authority before adaptive cells could be activated. This primordial faculty – the Innate immunity – operated using evolutionarily conserved pattern recognition receptors (PRR’s) rather than antibodies, and in hindsight simply explains why a person can be very sick but show little lymphocyte activation on their serology printouts – its because the Innate immunity is already hard at work, and it decides when and how much lymphocyte activation it requires to defeat an infection, without causing self harm to the host.
There was the difference – self modulating and benevolent immune engagement, as opposed to brute synthetic activation derived from crude adjuvants. Immunologist’s dirty little secret - of ‘lacing’ vaccines with adjuvants - was now exposed. Janeway’s new model showed there were three signals necessary before T lymphocytes could be released into the fight. Thus, antigenic invasion triggers the following signals:
Signal 1: Activation of PRR’s on macophages and dendritic cells, followed by recognition and binding to antigens. Neutrophils assist in destroying antigens by acting independently.
Signal 2: Upregulation of co-stimulatory molecules and cytokines (triggered by the macrophages and dendritic cells), to prepare for B lymphocyte activation if required.
Signal 3: Elaboration of pro-inflammatory cytokines to form and activate B cells, which then guide new and existing T lymphocytes into elite specialised killing forces.
Thus, the orthodox immunology establishment got a big lesson in how the primordial immune system functioned, and that tampering with those delicate protocols was unwise. Although Janeway’s discoveries have led to some new vaccine recipes which utilize PRR’s rather than adjuvants, amazingly, the brutal practice of adjuvanted immunology still prevails today together with the devastating injuries they incite. The whistle-blowing of Janeway and later, Gherardi (2003), and others appear to have been ignored by the pharmaceutical engine and health bureaucracies alike, because we find in the immunology literature numerous studies which persist in lymphocyte stimulation with the view to cornering some chemical device to be sold as an anti-disease vaccine. Thus, in the decade after Janeway’s passing, the reader still can witness questionable practices such as:
Immunophenotyping, antigen independent stimulation, cytokine driven changes, altered expression, polyclonal cell activation, stimulation triggering, cytokine stimulation, induced cytotoxicity, activated phenotype, selective expansion, coordinated induction, insertion cloning, high dose therapy, tumour blockading, genetic engineering, sustained secretion, modulation and modification; recombinant technology, genetically modified antigen, haptenated antigen, delivery of antigen-encoding genes, virus-derived vectors, and so on.
Yesterday and today’s adjuvanted immunology is as much alive and crude and toxic to human biology, as coal-fired energy is to the biosphere when compared to solar power. Equally extraordinary, is the strangle-hold that health authorities have maintained over public medical knowledge. While using their persuasive methods backed by government money to incite civil obedience, health authorities continue to ignore the ethics of adjuvanted reverse immunisation thereby demonstrating a knowledge of human immunity that could only be described as callous and indifferent.
Herein the author would suggest that Janeway’s whistle-blowing was rather modest when we consider other vaccine ingredients, which regretfully also include equally dangerous additives such as genetically modified organisms (GMO’s), phthalates, and mercury preservatives. Thus, the deployment of adjuvanted – GM pathogen vaccines represents a brute ‘one size fits all approach’ which offers no sensitivity for genotypic individuality whatsoever, and no compliance to a dedicated Innate-driven immune system. As such, non-native GM vaccines have not co-evolved with humans over millennia, but have been manufactured within extremely short periods using unnatural processes, and then released into the human gene pool with the naïve expectation that the human genome will adapt ‘overnight’. Rather than being just one secret, we would be well placed to expand Janeway’s phrase to: ‘Immunologist’s dirty little secrets’ (plural) – trade secrets which health agencies and bureaucrats have traditionally kept the public in the dark over.
Innate pioneer Ruslan Medzhitov, a colleague who helped Janeway rewrite the immune model, and who took over Janeway’s position as professor of immunology at Yale University; offered some revealing comments concerning vaccination efficacy. In his review of recent immunological discoveries, Medzhitov (2009, 776-75) concluded his paper with the following statement about protective immunity:
“Here we know very little, and this in part explains our continuous failures in developing new effective vaccines. Once the principles of protective immunity are understood, we may finally be able to deliver on the promise of defeating major infectious diseases with vaccination. But then again, pathogens may have a different opinion on this matter”.
When interviewed two years later by DMM scientific editor Sarah Allan (2011, 430-2). Medzhitov reiterated his concerns by affirming the following:
“We now know a lot about immunogenicity….However, what we don’t know is how to induce a protective immune response – one that will provide protection from a given pathogen. And, because we don’t know that, the majority of vaccine candidates don’t work. In cases where vaccines do work, I think it’s just a lucky coincidence, because in reality we don’t know how to design them…..we don’t know the rules…..A protective immune response is induced during most natural infections, which means that the mechanisms controlling protective immunity can be naturally engaged. But, when we immunize, we probably only mimic immunogenicity and not those protective mechanisms, which is why we often don’t induce protective immunity with a vaccine.”
The “different opinion” that Medzhitov referred to regarding the self defense survival capabilities of pathogens is a foregone conclusion. Pathogens are well known for their ability to develop resistance against human counter-measures. In medicine we havelong known of antibiotic resistance (Eg: TB, Golden Staff.) Why then do health authorities ignore the risks of mass vaccination and gene pool manipulation? We have for some time already witnessed the ‘fruits’ of vaccination campaigns, as seen lately in CDC and news reports of disease clusters simulating Polio, Measles, and Whooping Cough, etc – in fully vaccinated communities! The CDC has also reported a 50% increase in allergies amongst the USA’s 300 million people in recent years. We also see big increases in neurological diseases such as autism and MS.
What does this say about vaccination campaigns and the people who promote them? What does it say about ‘secrets’ and the ‘fruit’ they conceive, and the endless subterfuge required to keep them buried? Medzhitov’s concerns about past and present vaccine science are clearly well founded. Coming from a leading institute of immunology, one would think that vaccination campaigners would stop to listen. Considering that we live in an electronic world plastered with health warnings about the risks of smoking tobacco, the risks of alcoholism, the risks of obesity, the risks of excess sugar/salt/cholesterol, the risks of speeding, the risks of stress, the risks of narcotics, and so on…….Why don’t we hear from the same sources about the risks of vaccines, especially when manufactures declare lengthy side-effects from vaccines on their product information leaflets? What is it that exempts vaccines from the usual medical scrutiny and regulatory broadcasts?
Health authorities and pro-vaccine fraternities religiously refuse to admit that vaccination is a dangerous ‘forcing’ of the immune system into a strange ‘reverse’ manner of operation (much like driving a car to a destination but in reverse gear). That unnatural engaging of the Adaptive immunity has its downside – the potential exceeding of built in safety margins for self tolerance, and the induction of out-of-control cytotoxicity states that fail to switch off in genetically susceptible individuals. As biochemical counter-measures, orthodox vaccine ingredients represent a blunt non-tailored method of retaliation against disease, lacking inbuilt safety protocols and oblivious to immunogenic predispositions.
What all this means, is that there are many people in the health sector who are aware that the human immune system is susceptible to artificial stimulation and injury, by the application of these experimental practices. Worse still, the products of such experimentation are knowingly released to the general public in the face of dire warnings from expert scientists and public outcries. Despite the fragility and uniqueness of each person’s geno-chemical signature, mass reverse engineering of the human immune pool via the use of vaccines still proliferates, supported by a conceptual framework of defective social science. In fact, vaccination has become such an implacable ideology so as to strangle scientific objection and corrupt the ethics and articles of medicine and justice. Vaccination has become a social religion which people and governments blindly place their faith in. Television stations and newspapers generally support this ideology knowing the source and content of their license obligations and political affiliations, and are known to foster a climate of derogatory innuendo against anti-vaccine campaigners.
Unfortunately, it is not in the interests of medical careers or profits to publicise these grave dangers. Institutions, governments and cartels alike are gathered up in the tides of popularity, career money and business, fighting disease and profiteering from disease. Indemnity waivers are the ruse of choice to protect such institutions, routinely When however, cytotoxicity arises from vaccine backfires (as probability would predict given the insidious mode of operation of adjuvanted vaccines); authorities and administrators admit nothing / evade evidence / create pre-existing conditions / substitute reality with opinion / manipulate legislation / discredit victims and whistleblowers / employ mental sectioning laws as weapons / radicalize anti-vaccination groups / suppress public knowledge of vaccine toxicity / and undertake propaganda campaigns to stifle public backlash.
These actions are committed by those who wish to avoid liability and protect position, prestige and reputation – all of which are valuable assets to protect. When these practiced liars are exposed, their subterfuge is simply passed off as ‘errors in natural justice’, ‘erred towards bias’, ‘incorrect diagnosis’, ‘overlooked facts’, or some other dismissive jargon. Such is the misleading and deceptive conduct that transpires in courts and offices, which towers over victims and whistleblowers and their scientific evidence. Such is the radical loyalty towards vaccines and vaccinators, whose religion shows no compunction at misleading the public and rigging judicial hearings with subterfuge.
Despite commercial and career advancements in modern immunotherapy, the dangers of manipulating the human immune system should not be under-estimated. Vaccine ingredients add new instructions to an individual’s genetic program, thus changing and/or damaging their birth program. The tragic deaths of hundreds of the innocent and the defenseless soon after being vaccinated, is a poignant reminder to health officials, drug lords, and global entities; that the laws of genetic sensitivity reside in human function with absolute sovereignty, and to ignore their intrinsic fixture is to do so with callous disregard.
This Prologue now progresses to some general definitions of human immunity, followed by Section E: Discussion where the author’s serology evidence is analysed. It will be shown from this serology a mirror of the toxicity described above – the unnatural stimulation of the author’s immune system leading to immune dysregulation and out-of-control cytotoxicity that fails to switch off. Supporting this analysis are # Charles Janeway was lead author in the reference textbook Immunobiology: The Immune System in Health and Disease, This text is now in its 7th edition and posthumously re-titled as:
Murphy, K.M; Travers, P. and Walport, M. 2007. Janeway’s Immunobiology. 7th Edition. Garland Publishing, New York. ISBN 0-8153-4101-6
Definitions:
Adjuvants:
Adjuvants are traditionally foreign substances which function as irritants or activators of the immune system. They are a component of many vaccines and act as artificial stimulators of the human immune system, often inducing an inflammatory response. The theoretical purpose of adjuvants varies but includes 1) to absorb the antigen in solution 2) to produce depot formation at the injection site 3) to increase the level of antigen interaction in the blood stream 4) to potently stimulate the production of B lymphocyte antibodies 5) to speed up seroprotection. Adjuvants are not participating members of human evolutionary immune development, and therefore do not contain any inbuilt margins towards genetic safety and self tolerance.
Adjuvants may be divided into organic and inorganic types. The most commonly used adjuvants by far are the inorganic adjuvants, especially those of metallic origin. Primary among these are the aluminium salts commercially referred to as aluminium hydroxide [AI(OH)3], aluminium phosphate [AIPO4], and aluminium hydroxyphosphate sulfate [AAHS]. The most common of these is aluminium hydroxide, which is structurally identified as poorly crystalline aluminium oxyhydroxide [AIO(OH)], commonly known as the mineral boehmite (Hem and White. 1995, 249). Alum, or aluminium potassium sulfate [KAI(SO4)2.12H2O], has misleadingly been referred to as an adjuvant. Alum however, was traditionally used as a precipitating purifier of protein antigens, and its use has long been in decline due to variability in product results (Gupta and Rost 1995, 229). The efficacy of aluminium adjuvants depends upon preparation methods, antigen specificity, and clumping potential. Aluminium-containing vaccines include those vaccines for cancer, hepatitis A and B, HPV, influenza, Japanese encephalitis, meningitis, mumps, pertussis, pneumonia, polio, salmonella, and tetanus.
Less common are the organic adjuvants such as bacterial endotoxin (or the outer cell wall of gram negative bacteria), also called lipopolysaccharide (LPS); other microbial components collectively called PAMPs, short for ‘pathogen-associated molecular patterns; and the newly experimental group of human pattern recognition receptors (PRR’s). Adjuvants are not the only chemicals added to vaccines. Frequently added are preservatives like ethyl mercury and formaldehyde, and various stabilizers, all of which present potential health threats.
Herein the author would suggest that Janeway’s whistle-blowing was rather modest when we consider other vaccine ingredients, which regretfully also include equally dangerous additives such as genetically modified organisms (GMO’s), phthalates, and mercury preservatives. Thus, the deployment of adjuvanted – GM pathogen vaccines represents a brute ‘one size fits all approach’ which offers no sensitivity for genotypic individuality whatsoever, and no compliance to a dedicated Innate-driven immune system. As such, non-native GM vaccines have not co-evolved with humans over millennia, but have been manufactured within extremely short periods using unnatural processes, and then released into the human gene pool with the naïve expectation that the human genome will adapt ‘overnight’. Rather than being just one secret, we would be well placed to expand Janeway’s phrase to: ‘Immunologist’s dirty little secrets’ (plural) – trade secrets which health agencies and bureaucrats have traditionally kept the public in the dark over.
Innate pioneer Ruslan Medzhitov, a colleague who helped Janeway rewrite the immune model, and who took over Janeway’s position as professor of immunology at Yale University; offered some revealing comments concerning vaccination efficacy. In his review of recent immunological discoveries, Medzhitov (2009, 776-75) concluded his paper with the following statement about protective immunity:
“Here we know very little, and this in part explains our continuous failures in developing new effective vaccines. Once the principles of protective immunity are understood, we may finally be able to deliver on the promise of defeating major infectious diseases with vaccination. But then again, pathogens may have a different opinion on this matter”.
When interviewed two years later by DMM scientific editor Sarah Allan (2011, 430-2). Medzhitov reiterated his concerns by affirming the following:
“We now know a lot about immunogenicity….However, what we don’t know is how to induce a protective immune response – one that will provide protection from a given pathogen. And, because we don’t know that, the majority of vaccine candidates don’t work. In cases where vaccines do work, I think it’s just a lucky coincidence, because in reality we don’t know how to design them…..we don’t know the rules…..A protective immune response is induced during most natural infections, which means that the mechanisms controlling protective immunity can be naturally engaged. But, when we immunize, we probably only mimic immunogenicity and not those protective mechanisms, which is why we often don’t induce protective immunity with a vaccine.”
The “different opinion” that Medzhitov referred to regarding the self defense survival capabilities of pathogens is a foregone conclusion. Pathogens are well known for their ability to develop resistance against human counter-measures. In medicine we havelong known of antibiotic resistance (Eg: TB, Golden Staff.) Why then do health authorities ignore the risks of mass vaccination and gene pool manipulation? We have for some time already witnessed the ‘fruits’ of vaccination campaigns, as seen lately in CDC and news reports of disease clusters simulating Polio, Measles, and Whooping Cough, etc – in fully vaccinated communities! The CDC has also reported a 50% increase in allergies amongst the USA’s 300 million people in recent years. We also see big increases in neurological diseases such as autism and MS.
What does this say about vaccination campaigns and the people who promote them? What does it say about ‘secrets’ and the ‘fruit’ they conceive, and the endless subterfuge required to keep them buried? Medzhitov’s concerns about past and present vaccine science are clearly well founded. Coming from a leading institute of immunology, one would think that vaccination campaigners would stop to listen. Considering that we live in an electronic world plastered with health warnings about the risks of smoking tobacco, the risks of alcoholism, the risks of obesity, the risks of excess sugar/salt/cholesterol, the risks of speeding, the risks of stress, the risks of narcotics, and so on…….Why don’t we hear from the same sources about the risks of vaccines, especially when manufactures declare lengthy side-effects from vaccines on their product information leaflets? What is it that exempts vaccines from the usual medical scrutiny and regulatory broadcasts?
Health authorities and pro-vaccine fraternities religiously refuse to admit that vaccination is a dangerous ‘forcing’ of the immune system into a strange ‘reverse’ manner of operation (much like driving a car to a destination but in reverse gear). That unnatural engaging of the Adaptive immunity has its downside – the potential exceeding of built in safety margins for self tolerance, and the induction of out-of-control cytotoxicity states that fail to switch off in genetically susceptible individuals. As biochemical counter-measures, orthodox vaccine ingredients represent a blunt non-tailored method of retaliation against disease, lacking inbuilt safety protocols and oblivious to immunogenic predispositions.
What all this means, is that there are many people in the health sector who are aware that the human immune system is susceptible to artificial stimulation and injury, by the application of these experimental practices. Worse still, the products of such experimentation are knowingly released to the general public in the face of dire warnings from expert scientists and public outcries. Despite the fragility and uniqueness of each person’s geno-chemical signature, mass reverse engineering of the human immune pool via the use of vaccines still proliferates, supported by a conceptual framework of defective social science. In fact, vaccination has become such an implacable ideology so as to strangle scientific objection and corrupt the ethics and articles of medicine and justice. Vaccination has become a social religion which people and governments blindly place their faith in. Television stations and newspapers generally support this ideology knowing the source and content of their license obligations and political affiliations, and are known to foster a climate of derogatory innuendo against anti-vaccine campaigners.
Unfortunately, it is not in the interests of medical careers or profits to publicise these grave dangers. Institutions, governments and cartels alike are gathered up in the tides of popularity, career money and business, fighting disease and profiteering from disease. Indemnity waivers are the ruse of choice to protect such institutions, routinely When however, cytotoxicity arises from vaccine backfires (as probability would predict given the insidious mode of operation of adjuvanted vaccines); authorities and administrators admit nothing / evade evidence / create pre-existing conditions / substitute reality with opinion / manipulate legislation / discredit victims and whistleblowers / employ mental sectioning laws as weapons / radicalize anti-vaccination groups / suppress public knowledge of vaccine toxicity / and undertake propaganda campaigns to stifle public backlash.
These actions are committed by those who wish to avoid liability and protect position, prestige and reputation – all of which are valuable assets to protect. When these practiced liars are exposed, their subterfuge is simply passed off as ‘errors in natural justice’, ‘erred towards bias’, ‘incorrect diagnosis’, ‘overlooked facts’, or some other dismissive jargon. Such is the misleading and deceptive conduct that transpires in courts and offices, which towers over victims and whistleblowers and their scientific evidence. Such is the radical loyalty towards vaccines and vaccinators, whose religion shows no compunction at misleading the public and rigging judicial hearings with subterfuge.
Despite commercial and career advancements in modern immunotherapy, the dangers of manipulating the human immune system should not be under-estimated. Vaccine ingredients add new instructions to an individual’s genetic program, thus changing and/or damaging their birth program. The tragic deaths of hundreds of the innocent and the defenseless soon after being vaccinated, is a poignant reminder to health officials, drug lords, and global entities; that the laws of genetic sensitivity reside in human function with absolute sovereignty, and to ignore their intrinsic fixture is to do so with callous disregard.
This Prologue now progresses to some general definitions of human immunity, followed by Section E: Discussion where the author’s serology evidence is analysed. It will be shown from this serology a mirror of the toxicity described above – the unnatural stimulation of the author’s immune system leading to immune dysregulation and out-of-control cytotoxicity that fails to switch off. Supporting this analysis are # Charles Janeway was lead author in the reference textbook Immunobiology: The Immune System in Health and Disease, This text is now in its 7th edition and posthumously re-titled as:
Murphy, K.M; Travers, P. and Walport, M. 2007. Janeway’s Immunobiology. 7th Edition. Garland Publishing, New York. ISBN 0-8153-4101-6
Definitions:
Adjuvants:
Adjuvants are traditionally foreign substances which function as irritants or activators of the immune system. They are a component of many vaccines and act as artificial stimulators of the human immune system, often inducing an inflammatory response. The theoretical purpose of adjuvants varies but includes 1) to absorb the antigen in solution 2) to produce depot formation at the injection site 3) to increase the level of antigen interaction in the blood stream 4) to potently stimulate the production of B lymphocyte antibodies 5) to speed up seroprotection. Adjuvants are not participating members of human evolutionary immune development, and therefore do not contain any inbuilt margins towards genetic safety and self tolerance.
Adjuvants may be divided into organic and inorganic types. The most commonly used adjuvants by far are the inorganic adjuvants, especially those of metallic origin. Primary among these are the aluminium salts commercially referred to as aluminium hydroxide [AI(OH)3], aluminium phosphate [AIPO4], and aluminium hydroxyphosphate sulfate [AAHS]. The most common of these is aluminium hydroxide, which is structurally identified as poorly crystalline aluminium oxyhydroxide [AIO(OH)], commonly known as the mineral boehmite (Hem and White. 1995, 249). Alum, or aluminium potassium sulfate [KAI(SO4)2.12H2O], has misleadingly been referred to as an adjuvant. Alum however, was traditionally used as a precipitating purifier of protein antigens, and its use has long been in decline due to variability in product results (Gupta and Rost 1995, 229). The efficacy of aluminium adjuvants depends upon preparation methods, antigen specificity, and clumping potential. Aluminium-containing vaccines include those vaccines for cancer, hepatitis A and B, HPV, influenza, Japanese encephalitis, meningitis, mumps, pertussis, pneumonia, polio, salmonella, and tetanus.
Less common are the organic adjuvants such as bacterial endotoxin (or the outer cell wall of gram negative bacteria), also called lipopolysaccharide (LPS); other microbial components collectively called PAMPs, short for ‘pathogen-associated molecular patterns; and the newly experimental group of human pattern recognition receptors (PRR’s). Adjuvants are not the only chemicals added to vaccines. Frequently added are preservatives like ethyl mercury and formaldehyde, and various stabilizers, all of which present potential health threats.
The ubiquitous use of metallic salts to act as immune stimulators represents a crude and blunt approach of ‘forcing’ seroprotection in a reverse manner to the natural sequence of immune acquisition. Accompanying their ability to induce inflammatory responses in their hosts is their potential to cause irreversible damage, this demonstrated by massive inflammations and disturbances to the physiology of genetically susceptible people, which we casually label as ‘vaccine reactions’. Injuries can include lymphadenopathy, fever, inflammatory neurologies, eosinophilia, antigenicity failure, myalgia, chronic fatigue, organ-specific toxicity, irritable digestive disorders, mobility disorders, blood abnormalities, paralysis, and death.
Yale Professor of Immunology Charles Janeway (1989) questioned the ethics of adjuvant use, describing the practice as ‘Immunologist’s dirty little secret’. In 2003, French researchers named aluminium hydroxide adjuvants as the cause of vaccine induced macrophagic myofascitis (MMF) – a disorder involving muscle pain, neurologies and chronic fatigue (Gherardi, 2003). To date, Gherardi’s findings have not been successfully challenged.
Antibodies:
Are specific immunoglobulins made by B lymphocytes of the Adaptive immunity, which act as a memory reservoir for future exposure. Some antibodies are lifelong (eg: Hepatitis, Mumps, Measles, etc); while other antibodies are short lived (eg: Acute term infections such as Colds, Influenzas; and many vaccine-mediated antibodies). There are five antibody isotypes generated by the humoral (B) lymphocytes:
Immunoglobulin A – (IgA): mucosal antibodies in the lungs, GIT, and the skin.
Immunoglobulin D – (IgD): antibody receptors bound onto naïve B cells.
Immunoglobulin E – (IgE): antibodies bound onto allergens triggering histamines.
Immunoglobulin M – (IgM): short term serum antibodies for acute phase exposure.
Immunoglobulin G – (IgG): long term serum antibodies for chronic/past exposure.
Antigenicity: (Antibody – generating – ability)
In layman’s terms, antigenicity simply means ‘acquired immunity to a disease’. In traditional biological terms, antigenicity means the quality or measure of memory recognition resistance (ie: immunity) against a specific antigen, after initial exposure to that antigen has been overcome.
Acquired antigenicity is the function of the Adaptive immunity via the production of B cell antibodies and T cell receptors. The degree and duration of antigenicity depends upon the type and dose of antigen (organic or inorganic), the genotypic capacity and sensitivity of the individual host, the originality of the antigen (naturally occurring or artificially modified), and the pathways of exposure to the antigen (by natural contact, inhalation or ingestion; or by artificial inoculation or delivery). Some human gene pools who have never been exposed to certain antigens, (eg: small pox and influenza introductions to non-European colonies), can decimate those populations – as history has demonstrated.
Antigenicity varies greatly between natural exposures to environmentally conserved antigens (such as traditional diseases), and artificially delivered exposures to modified antigens. For example, natural exposure to hepatitis / measles / pox pathogens usually confers life-long antigenicity, but vaccinated exposure to these pathogens regularly produces short or zero antigenicity, requiring repeat boosters. Thus, true antigenicity (or immunity) imparts the property of long term memory that is genetically stylized to each individual’s biochemical signature.
While antigenicity is the function of the Adaptive immunity, it does not constitute the sole immune response to subsequent exposure to similar antigens. Repeat exposure to any antigen will normally involve the Innate immunity as well, which signals its instructions to the Adaptive immunity as required.
Immunogenicity:
This is a more recent term which encompasses the same meaning as antigenicity, with both terms having been used interchangeably. However, immunogenicity also includes the wider immune responses provoked by antigens involving the Innate immunity and the genetic under-frame of immunity, as well as the Adaptive immunity. Since genes and immunity share a cooperative inter-dependency, so immunogenicity must also incorporate the total and wider immune responses to antigens, other than antibody production alone.
For example, many therapeutic drugs are known to provoke unwanted immune responses in people, leading to adverse events and subsequent civil lawsuits. Some of these adverse events include unwanted genetic changes to individuals. Clinically relevant immunogenic responses include vaccine adverse events leading to chronic injury, the activation of anti-drug antibodies (ADA), and the onset of drug induced events such as food intolerances, blood changes, tissue damage, neurological damage, etc, and death. The onset of drug-related side-effects is very much a function of immunogenicity, and not just physiology alone. Thus, when a vaccine produces an immunogenic response, that response may include unwanted and long term changes to immunity. Therefore, there is sound scientific basis for equating unwanted immunogenicity with safety concerns.
Immune System:
Is an integrated network of organs, glands, marrows and fluids; which regulates and protects much of the body’s operating systems. It is divided into two defense faculties: 1) the non-specific recognition (Innate) immunity and, 2) the acquired specific recognition (Adaptive) immunity. The immune system, like all body systems, is underwritten by the genetic constitution of each host, whose genetic complement and expression is specific to each individual. The fluidic immunity consists of a variety of Leukocytes – commonly known as white blood cells (WBC) which are divided between the Innate and Adaptive faculties. Most WBC subpopulations belong to the more ancient Innate immunity and include neutrophils, NK lymphocytes, monocytes, eosinophils and basophils. The Innate immunity does not confer extended antigenicity to the host. The Adaptive immunity consists of B and T lymphocytes only, and these do acquire extended antigenicity. The Innate immunity is the dominant command structure and first responder to antigen exposure, and it decides whether to marshal extra assistance from the Adaptive immunity when needed. When provoked, immune system counter measures may take the form of one or more of the following responses:
o an Allergenic response: the generation of a rapid hypersensitivity reaction.
o an Antibody response: the generation of specific immunoglobulins to infection.
o an Anti-Immunoglobulin response: where immune proteins attack antibodies.
o an Autogenic response: an autoimmune cytotoxic generation against ‘self’.
o an Immunogenic response: a substance that generates any immune response.
o a Pathogenic response: an intolerance generated to antigens of various types.
o a Tolerogenic response: a substance that generates a non-response or suppression.
Pattern Recognition Receptors (PRR): These are small specialised proteins secreted on the surface of Innate cells, which sense antigens in generic ways. After recognizing antigens, Innate cells bind to the invaders to destroy them, while triggering cytokine releases to attract more help from other immune cells. Families of PRR include Toll-like receptors (TLR), Nod-like receptors (NLR), Cytosolic receptors, Collectins, Ficelins, Pentraxins, Inflammasome complexes, LPS complexes, and RIG-1 / MDA-5 / and MBA types. More families are being discovered.
Protective Immunity:
This is an alternative term having the same meaning as true antigenicity. When pathogens are remembered by the host’s immune system, such memory is usually acquired after natural environmental exposure to antigens via the ear-nose-throat pathway. Four types of immune cells have memory. These are macrophages and dendritic cells belonging to the Innate immunity, and B cells and some mature T helper cells of the Adaptive immunity. The first three types are called antigen presenting cells (APC’s), as they can carry the protein marker of some antigens on their surfaces which they can present to other immune cells to initiate attack and destroy operations. Natural exposures provoke protective immunity of different durations however. Innate cells produce short immunity of only hours or days, while long term immunity is produced from B lymphocyte cells which possess adaptive memory.
As stated above under the heading antigenicity, true protective immunity depends upon genotypically written memory formulated within each human host as host cells interface with invading antigens, which then lock in specific memory formulations. Each person possesses their own genotypically written memory-immunity, which works best for them when re-exposed to same or similar antigens. This explains why some people acquire long term immunity to (for example) influenza viruses, while other people die from the same virus. The bulk of people however, reside somewhere in between these two extremes, having to fight influenza infections for 1 to 3 weeks before beating it. With polio, some 90% of people never know they’ve had it, while less than 1% will suffer crippling symptoms. In other words, we see genotypic immunity ranging from robust – to moderate – to highly sensitive. Individually tailored immunity is the ideal parameter for protective antigenicity.
We also see genomic immunity where humans display good resistance to some pathogens, but not to others. For example, the human gut is highly susceptible to salmonella, but reptiles and birds readily tolerate salmonella. There are many animal diseases which do not harm human immunity, but there are some which do, such as bird flu, rabies, and bat viruses.
Recent events in west Africa involving the Ebola virus have demonstrated globally that immunity can be ‘swapped’ from one individual to another, just as certain blood types can be shared. To date, human resilience against the Ebola virus in under-developed countries has shown itself to be disturbingly low, demonstrated by a 40% mortality rate reported in news media. As with all diseases, some human genotypes manage to beat the disease while other genotypes succumb and perish. Out of this struggle for survival however, it has been demonstrated that antibodies developed within survivors of the virus, can be extracted and donated to others who are struggling with their own infections. Thus, donated genome-specific pre-nurtured antibodies represent an amenable method of disease control, because such antibodies are tailored for the human genome by the human genome, without chemical additives or genetically engineered inclusions.
White Blood Cells: (Leukocytes):
– Sub-sets: A): Myeloids B): Lymphocytes
A): Myeloids: These are the largest group of leukocytes and make up the bulk of
the Innate immunity. The myeloid family consists of the following cell types:
Þ Neutrophils: Are the most abundant family of defense cell in the innate immune system, comprising about 50-70% of the WBC compliment in human blood. They are short lived, highly motile cells, filled with microscopic sacs (or granules) containing enzymes that digest antigens. Given this internal structure, they are also called Neutrophil granulocytes, and are the first responders to infection or inflammation. Neutrophils are therefore the benchmark signaler of immune activation to internal disturbance. Given their Innate status, their non-specificity permits them to respond and destroy any pathogen or substance that they regard should not be in the body, without going through pre-recognition phases. They are subdivided into 1) Segmented neutrophils [or segs]; 2) Banded neutrophils [or bands]. Testing can be done from an ‘Absolute Neutrophil Count’ (ANC) test, or Full Blood Count (FBC).
Þ Monocytes: Are the largest of all leukocytes, are comparatively long lived, and belong to the innate immunity. New monocytes develop into three main phenotypes of CD14 and CD16 cell surface receptors, these being: 1) Classical 2) Non-classical, and 3) Intermediate types. Monocytes have a variety of roles including antigen destruction and signaling to other immune cells. Older monocytes migrate into various body tissues where they differentiate into Macrophages or Dendritic cells:-
Macrophages: Meaning ‘big eaters’, these are large cells comprising about 2-10% of leukocytes. Macrophages are mature monocytes which leave the blood to take up residence in many organs and tissues, where they differentiate into their final macrophage phase. They are classified into two phenotypic groups, called killer macrophages (M1) and repair macrophages (M2), depending on the number of proteins each phenotype expresses. Their role is to digest foreign material and microbial pathogens; to remove senile o cells and cellular debris; to assist tissue repair and regeneration; and to present antigens to other immune cells. In an undisturbed immune system macrophages are programmed to be host friendly, but they can attack a host’s own muscle tissue if reprogrammed by vaccine components, resulting in the condition called macrophagic myofasciitis.
o Dendritic Cells: Are older monocytes which have evolved into potent messenger and courier cells, which specialise in presenting antigens to T cells. Their ability to interact between the Innate and Adaptive immune faculties, lends credence to their naming as ‘accessory cells’. They are the only antigen-presenting cell which can activate both memory and naïve T cells. Dendritic cells reside in lymph nodes and external tissues (such as the nose, lungs, skin, & GIT).
Þ Eosinophils: Activate and mediate allergic type IgE reactions such as hayfever, asthma, hives, insect stings, and parasitic infections.
Þ Basophils: Activate allergic type IgE reactions, releasing histamines.
B): Lymphocytes: These are the second most abundant family of defense cell in
the immune system, comprising about 20-40% of total leukocytes. Types include
the Humoral (B cells), and the Cellular (T cells and NK cells). Excluding NK
cells, the B and T lymphocytes make up the Adaptive immunity.
Þ B Cells: These produce antibodies for the Adaptive immunity by targeting antigens for destruction, then present them to T cells.
Þ T Cells: Also belong to the Adaptive immunity. Some regulate immune responses, while others destroy antigens.
Þ NK Cells: Natural Killers belong to the Innate immunity. They are toxic to antigens without need for pre-recognition/arming protocols.
Leukocytosis: Where White Cell Count (WCC) passes above 10.0 x10^9 / L. There are a variety of causes for this condition, including immune reactions to toxins and drugs. WCC range parameters are normally 3.5-10.0 ^9 / L.
Neutrophilia: Where the neutrophil portion of WCC increases above 70% of the total. There are a variety of causes for neutrophilia, including immune reactions to drugs (including vaccines), and exposure to microbial pathogens.
Lymphopenia: Where the lymphocyte portion of WCC decreases below 20% of the total. Lymphocyte reduction often occurs in commensurate response to neutrophil increases.
Yale Professor of Immunology Charles Janeway (1989) questioned the ethics of adjuvant use, describing the practice as ‘Immunologist’s dirty little secret’. In 2003, French researchers named aluminium hydroxide adjuvants as the cause of vaccine induced macrophagic myofascitis (MMF) – a disorder involving muscle pain, neurologies and chronic fatigue (Gherardi, 2003). To date, Gherardi’s findings have not been successfully challenged.
Antibodies:
Are specific immunoglobulins made by B lymphocytes of the Adaptive immunity, which act as a memory reservoir for future exposure. Some antibodies are lifelong (eg: Hepatitis, Mumps, Measles, etc); while other antibodies are short lived (eg: Acute term infections such as Colds, Influenzas; and many vaccine-mediated antibodies). There are five antibody isotypes generated by the humoral (B) lymphocytes:
Immunoglobulin A – (IgA): mucosal antibodies in the lungs, GIT, and the skin.
Immunoglobulin D – (IgD): antibody receptors bound onto naïve B cells.
Immunoglobulin E – (IgE): antibodies bound onto allergens triggering histamines.
Immunoglobulin M – (IgM): short term serum antibodies for acute phase exposure.
Immunoglobulin G – (IgG): long term serum antibodies for chronic/past exposure.
Antigenicity: (Antibody – generating – ability)
In layman’s terms, antigenicity simply means ‘acquired immunity to a disease’. In traditional biological terms, antigenicity means the quality or measure of memory recognition resistance (ie: immunity) against a specific antigen, after initial exposure to that antigen has been overcome.
Acquired antigenicity is the function of the Adaptive immunity via the production of B cell antibodies and T cell receptors. The degree and duration of antigenicity depends upon the type and dose of antigen (organic or inorganic), the genotypic capacity and sensitivity of the individual host, the originality of the antigen (naturally occurring or artificially modified), and the pathways of exposure to the antigen (by natural contact, inhalation or ingestion; or by artificial inoculation or delivery). Some human gene pools who have never been exposed to certain antigens, (eg: small pox and influenza introductions to non-European colonies), can decimate those populations – as history has demonstrated.
Antigenicity varies greatly between natural exposures to environmentally conserved antigens (such as traditional diseases), and artificially delivered exposures to modified antigens. For example, natural exposure to hepatitis / measles / pox pathogens usually confers life-long antigenicity, but vaccinated exposure to these pathogens regularly produces short or zero antigenicity, requiring repeat boosters. Thus, true antigenicity (or immunity) imparts the property of long term memory that is genetically stylized to each individual’s biochemical signature.
While antigenicity is the function of the Adaptive immunity, it does not constitute the sole immune response to subsequent exposure to similar antigens. Repeat exposure to any antigen will normally involve the Innate immunity as well, which signals its instructions to the Adaptive immunity as required.
Immunogenicity:
This is a more recent term which encompasses the same meaning as antigenicity, with both terms having been used interchangeably. However, immunogenicity also includes the wider immune responses provoked by antigens involving the Innate immunity and the genetic under-frame of immunity, as well as the Adaptive immunity. Since genes and immunity share a cooperative inter-dependency, so immunogenicity must also incorporate the total and wider immune responses to antigens, other than antibody production alone.
For example, many therapeutic drugs are known to provoke unwanted immune responses in people, leading to adverse events and subsequent civil lawsuits. Some of these adverse events include unwanted genetic changes to individuals. Clinically relevant immunogenic responses include vaccine adverse events leading to chronic injury, the activation of anti-drug antibodies (ADA), and the onset of drug induced events such as food intolerances, blood changes, tissue damage, neurological damage, etc, and death. The onset of drug-related side-effects is very much a function of immunogenicity, and not just physiology alone. Thus, when a vaccine produces an immunogenic response, that response may include unwanted and long term changes to immunity. Therefore, there is sound scientific basis for equating unwanted immunogenicity with safety concerns.
Immune System:
Is an integrated network of organs, glands, marrows and fluids; which regulates and protects much of the body’s operating systems. It is divided into two defense faculties: 1) the non-specific recognition (Innate) immunity and, 2) the acquired specific recognition (Adaptive) immunity. The immune system, like all body systems, is underwritten by the genetic constitution of each host, whose genetic complement and expression is specific to each individual. The fluidic immunity consists of a variety of Leukocytes – commonly known as white blood cells (WBC) which are divided between the Innate and Adaptive faculties. Most WBC subpopulations belong to the more ancient Innate immunity and include neutrophils, NK lymphocytes, monocytes, eosinophils and basophils. The Innate immunity does not confer extended antigenicity to the host. The Adaptive immunity consists of B and T lymphocytes only, and these do acquire extended antigenicity. The Innate immunity is the dominant command structure and first responder to antigen exposure, and it decides whether to marshal extra assistance from the Adaptive immunity when needed. When provoked, immune system counter measures may take the form of one or more of the following responses:
o an Allergenic response: the generation of a rapid hypersensitivity reaction.
o an Antibody response: the generation of specific immunoglobulins to infection.
o an Anti-Immunoglobulin response: where immune proteins attack antibodies.
o an Autogenic response: an autoimmune cytotoxic generation against ‘self’.
o an Immunogenic response: a substance that generates any immune response.
o a Pathogenic response: an intolerance generated to antigens of various types.
o a Tolerogenic response: a substance that generates a non-response or suppression.
Pattern Recognition Receptors (PRR): These are small specialised proteins secreted on the surface of Innate cells, which sense antigens in generic ways. After recognizing antigens, Innate cells bind to the invaders to destroy them, while triggering cytokine releases to attract more help from other immune cells. Families of PRR include Toll-like receptors (TLR), Nod-like receptors (NLR), Cytosolic receptors, Collectins, Ficelins, Pentraxins, Inflammasome complexes, LPS complexes, and RIG-1 / MDA-5 / and MBA types. More families are being discovered.
Protective Immunity:
This is an alternative term having the same meaning as true antigenicity. When pathogens are remembered by the host’s immune system, such memory is usually acquired after natural environmental exposure to antigens via the ear-nose-throat pathway. Four types of immune cells have memory. These are macrophages and dendritic cells belonging to the Innate immunity, and B cells and some mature T helper cells of the Adaptive immunity. The first three types are called antigen presenting cells (APC’s), as they can carry the protein marker of some antigens on their surfaces which they can present to other immune cells to initiate attack and destroy operations. Natural exposures provoke protective immunity of different durations however. Innate cells produce short immunity of only hours or days, while long term immunity is produced from B lymphocyte cells which possess adaptive memory.
As stated above under the heading antigenicity, true protective immunity depends upon genotypically written memory formulated within each human host as host cells interface with invading antigens, which then lock in specific memory formulations. Each person possesses their own genotypically written memory-immunity, which works best for them when re-exposed to same or similar antigens. This explains why some people acquire long term immunity to (for example) influenza viruses, while other people die from the same virus. The bulk of people however, reside somewhere in between these two extremes, having to fight influenza infections for 1 to 3 weeks before beating it. With polio, some 90% of people never know they’ve had it, while less than 1% will suffer crippling symptoms. In other words, we see genotypic immunity ranging from robust – to moderate – to highly sensitive. Individually tailored immunity is the ideal parameter for protective antigenicity.
We also see genomic immunity where humans display good resistance to some pathogens, but not to others. For example, the human gut is highly susceptible to salmonella, but reptiles and birds readily tolerate salmonella. There are many animal diseases which do not harm human immunity, but there are some which do, such as bird flu, rabies, and bat viruses.
Recent events in west Africa involving the Ebola virus have demonstrated globally that immunity can be ‘swapped’ from one individual to another, just as certain blood types can be shared. To date, human resilience against the Ebola virus in under-developed countries has shown itself to be disturbingly low, demonstrated by a 40% mortality rate reported in news media. As with all diseases, some human genotypes manage to beat the disease while other genotypes succumb and perish. Out of this struggle for survival however, it has been demonstrated that antibodies developed within survivors of the virus, can be extracted and donated to others who are struggling with their own infections. Thus, donated genome-specific pre-nurtured antibodies represent an amenable method of disease control, because such antibodies are tailored for the human genome by the human genome, without chemical additives or genetically engineered inclusions.
White Blood Cells: (Leukocytes):
– Sub-sets: A): Myeloids B): Lymphocytes
A): Myeloids: These are the largest group of leukocytes and make up the bulk of
the Innate immunity. The myeloid family consists of the following cell types:
Þ Neutrophils: Are the most abundant family of defense cell in the innate immune system, comprising about 50-70% of the WBC compliment in human blood. They are short lived, highly motile cells, filled with microscopic sacs (or granules) containing enzymes that digest antigens. Given this internal structure, they are also called Neutrophil granulocytes, and are the first responders to infection or inflammation. Neutrophils are therefore the benchmark signaler of immune activation to internal disturbance. Given their Innate status, their non-specificity permits them to respond and destroy any pathogen or substance that they regard should not be in the body, without going through pre-recognition phases. They are subdivided into 1) Segmented neutrophils [or segs]; 2) Banded neutrophils [or bands]. Testing can be done from an ‘Absolute Neutrophil Count’ (ANC) test, or Full Blood Count (FBC).
Þ Monocytes: Are the largest of all leukocytes, are comparatively long lived, and belong to the innate immunity. New monocytes develop into three main phenotypes of CD14 and CD16 cell surface receptors, these being: 1) Classical 2) Non-classical, and 3) Intermediate types. Monocytes have a variety of roles including antigen destruction and signaling to other immune cells. Older monocytes migrate into various body tissues where they differentiate into Macrophages or Dendritic cells:-
Macrophages: Meaning ‘big eaters’, these are large cells comprising about 2-10% of leukocytes. Macrophages are mature monocytes which leave the blood to take up residence in many organs and tissues, where they differentiate into their final macrophage phase. They are classified into two phenotypic groups, called killer macrophages (M1) and repair macrophages (M2), depending on the number of proteins each phenotype expresses. Their role is to digest foreign material and microbial pathogens; to remove senile o cells and cellular debris; to assist tissue repair and regeneration; and to present antigens to other immune cells. In an undisturbed immune system macrophages are programmed to be host friendly, but they can attack a host’s own muscle tissue if reprogrammed by vaccine components, resulting in the condition called macrophagic myofasciitis.
o Dendritic Cells: Are older monocytes which have evolved into potent messenger and courier cells, which specialise in presenting antigens to T cells. Their ability to interact between the Innate and Adaptive immune faculties, lends credence to their naming as ‘accessory cells’. They are the only antigen-presenting cell which can activate both memory and naïve T cells. Dendritic cells reside in lymph nodes and external tissues (such as the nose, lungs, skin, & GIT).
Þ Eosinophils: Activate and mediate allergic type IgE reactions such as hayfever, asthma, hives, insect stings, and parasitic infections.
Þ Basophils: Activate allergic type IgE reactions, releasing histamines.
B): Lymphocytes: These are the second most abundant family of defense cell in
the immune system, comprising about 20-40% of total leukocytes. Types include
the Humoral (B cells), and the Cellular (T cells and NK cells). Excluding NK
cells, the B and T lymphocytes make up the Adaptive immunity.
Þ B Cells: These produce antibodies for the Adaptive immunity by targeting antigens for destruction, then present them to T cells.
Þ T Cells: Also belong to the Adaptive immunity. Some regulate immune responses, while others destroy antigens.
Þ NK Cells: Natural Killers belong to the Innate immunity. They are toxic to antigens without need for pre-recognition/arming protocols.
Leukocytosis: Where White Cell Count (WCC) passes above 10.0 x10^9 / L. There are a variety of causes for this condition, including immune reactions to toxins and drugs. WCC range parameters are normally 3.5-10.0 ^9 / L.
Neutrophilia: Where the neutrophil portion of WCC increases above 70% of the total. There are a variety of causes for neutrophilia, including immune reactions to drugs (including vaccines), and exposure to microbial pathogens.
Lymphopenia: Where the lymphocyte portion of WCC decreases below 20% of the total. Lymphocyte reduction often occurs in commensurate response to neutrophil increases.

E): ANALYSIS and DISCUSSION of RESULTS: the DAMAGE:
This Section is divided into the following parts:
Ø Part 1: NEUROLOGY PATHOLOGIES:
- NCV findings
Ø Part 2: IMAGING PATHOLOGIES:
- Ultrasound findings
- CT Scan findings
- MRI Scan findings
Ø Part 3: BODY FLUID PATHOLOGIES:
- Liver Enzyme Disruption
- Pathogenic Sensitivity Screening
- ESR/CRP/UMC/FB Non-specific Screening
- Pre-existing Conditions Screening - Total White Blood Cell Count Reactivity
- White Blood subsets: Neutrophils and Lymphocytes
- Lymphocyte Subsets: Autoimmune Dysregulation
Ø Part 4: OVERVIEW AT THE 5 YEAR MARKER.
Ø Part 1. NEUROLOGY PATHOLOGIES:
- NCV findings:
The human nervous system may be divided into the Central, Enteric, Peripheral, and Autonomic nervous systems. Injury to either system may result in a variety of symptoms to limbs, abdomen, or the head. If such injury arises, the services of a neurologist may be required to investigate the source and extent of any nerve damage. Many neurologists have reportedly shown reluctance in undertaking investigations for vaccine victims. To document vaccine damage could invite scorn from one’s peers and jeopardy to one’s career, as some health agencies regard this help as dissent.
A condition of low grade paralysis had occurred in the author’s legs in the first three months of illness (the acute phase), where mobility was limited to about 10 steps to the toilet and return to bed. The legs were acutely weakened and woody. After the bed confinement had passed, the legs remained in a state of chronic weakness requiring a mobility frame for shopping excursions. Subsequent research revealed that leg disorders were a common symptom in the testimonies of vaccine injured victims.
Accordingly, a neurologist was consulted to investigate the author’s mobility problems. Despite a number of neurological tests being available, the neurologist undertook only one test, that being a Nerve Conduction Velocity test (NCV). This simple electrical test measures straight line conductivity of electrical impulses as they are transmitted along nerve bundles, primarily from point A to point B. Decreases in the velocity of impulses at normal body temperatures, may indicate nerve disease or injury to muscle function. NCV tests help identify conditions such as Guillaine-barre syndrome, carpal tunnel, Charcot-Marie tooth disease, herniated disc disease, chronic inflammatory polyneuropathy and neuropathy, sciatic nerve complaints, pinched or crushed nerves, and Peripheral injuries including numbness and tingling or itching.
The NCV test was undertaken on the 08 April 2010, about one year after the onset of illness, during the Intermediate phase of the injury. The test was performed on the legs while at rest in the seated position. There were no conduction irregularities cited by the neurologist from this test at that time. No further neurological tests have been followed up or recommended by the neurologist, despite persisting leg weakness.
The potential deficiency in the NCV test was that conduction was measured only between two points primarily along a major nerve bundle, without reference to the capacities of numerous lateral nerve synapses. The deficiency of the NCV test undertaken becomes apparent in that it does not measure ‘strain’ (or load). It does not measure the leg weakness the author feels first thing out of bed, or the strain after walking short distances of 50 to 75 m using a wheelie walker. It also does not measure the particular ‘woodiness’ the author has felt when prompted to skip a few metres to avoid an oncoming vehicle, whereas prior to vaccination the legs could run swiftly and fluidly without any impedance. These are loads not measured by the NCV test.
The fact that involuntary muscle tremors were experienced for 2 years reducing to episodic spasms, and that chronic weakening of the legs occurred requiring a mobility frame, strongly suggests the onset of a neuromuscular disorder following vaccination.
Ø Part 2. IMAGING PATHOLOGIES:
- Ultrasound findings
- CT Scan and MRI Scan findings
Chronology: 1st Ultrasound - 02. 06. 2009 Abdomen.
2nd Ultrasound - 30. 09. 2009 Abdomen.
1st CT Scan - 08. 01. 2010 Lumbar Spine.
1st MRI Scan - 11. 10. 2010 Abdomen.
3rd Ultrasound - 01. 09. 2011 Abdomen.
4th Ultrasound - 01. 02. 2012 Scrotum.
The 1st Ultrasound results found that: “The liver shows moderate fatty changes as well as enlargement of the left lobe and the caudate lobe” (02.06. 2009). The occurrence of this sudden and acute liver inflammation (ie: a hepatitis condition) for several months after the 2nd inoculation, was one of the early pieces of evidence that demonstrated that a significant injury was in progress, for which there were no contributing lifestyle factors (ie: no fatty diets, no fast foods, no alcoholic habits, no lethargic habits, and no identifiable pathogens). This first abdominal investigation was performed some 12 weeks after the 2nd inoculation, when the author was 50 years old. The findings of this ultrasound supports the proposition for this study that the vaccine solely caused the author’s injury, including the liver inflammation noted here.
The 2nd Ultrasound undertaken on 30.09.09, a further 12 weeks after the first ultrasound, found no visible liver abnormality remaining. The withdrawal of the swelling and fatty condition after the acute phase ended, further implicates vaccine causality for this transient hepatitis, rather than the condition being virally activated. Liver viremias are typified by persisting fatty infiltration which may be chronic for some years after infection passes. The fattiness of the author’s liver did not persist, indicating non-pathogenic disruption to liver histology.
The 1st MRI also showed that the visible structural injury to the liver was no longer visible despite continuing abdominal pain in the liver region. The MRI did not detect any lesions or cirrhosis of the liver, indicating that no chronic hepatic trauma had ever been sustained to the liver before vaccination (such as the effects of substance abuses). In other words, the author’s liver was in excellent condition before the post- vaccination “enlargement” occurred.
The 3rd Ultrasound gave the same results as the 2nd, indicating no abnormalities at the focal / structural plane, and no reversion back to acute phase pathologies. The 4th Ultrasound detected no focal abnormalities to the testes, the scrotal pain most likely representing diffuse myalgia often associated with post-vaccination pathologically induced neuromuscular disorder.
The CT Scan of the lower back demonstrated no disc protrusions, no nerve entrapments, and no vertebral compression at any level, indicating no spinal inflammatory hereditary conditions. There was detected only mild degenerative change between 3 vertebrae, indicating the normal effects of physical labour over time in combination with deterioration associated with aging. The back pain which prompted this test may have been an artifact of the Acute and Intermediate phase symptoms, as the author did not usually suffer from persisting back pain before vaccination.
Thus, as noted above, the primary injury visible from the imaging tests was to the liver. The 1st Ultrasound confirmed that a structural injury occurred to the liver soon after vaccination, namely swelling and fatty reactions, which remained for a limited period of some 3-5 months. The 2nd Ultrasound concluded that the swelling and fattiness had subsided. Serology confirmed that disruption to the liver was of non-pathogenic origin. Serology also confirmed that large amounts of liver enzymes were released into the bloodstream at the time of the enlargement, and that those releases remained abnormally high or erratic before settling about 3 to 3.5 years after the inoculations were given (see next section). The liver reaction is therefore best described as a Toxic Hepatitis, a condition known to occur as a result of the adverse impression certain drugs create upon human physiology – in this case the vaccine.
Regulated serum release of liver enzymes within normal range parameters, is part of the normal maintenance process of non-inflammatory gradual cell death (apoptosis) and cell replacement. However, large enzyme releases into the bloodstream, as is noted in the author’s test results, are typically a sign of inflammatory and premature cell death of hepatocytes (liver cells). In other words, an apoptotic cascade occurred following vaccination, explaining why inflammation of the liver lobes became visible to the ultrasound. This enlargement signifies that a sudden cascade of cell death of massive proportions took place over several months, for which no pathogen could be identified. Inflammation is the primary source of pain and discomfort, and accounts for the RHS abdominal pain associated with this injury.
Despite the eventual subsidence of the enzymes after 3+ years, and the lack of any bile duct obstructions in subsequent scans, daily RHS abdominal pain has persisted to the 5 year marker indicating that long term injury to the liver has probably occurred. Lipski (2012, 20, 237) noted that the liver can lose as much as 70% of its capability and not show diagnosable data indicating liver disease, and that if the immune system attacks the liver, it is probably due to a genetic defect.
That ‘defect’ has been the subject of much scholarly investigation and in the case of vaccine-induced injury states, represents a chemically induced defect caused by the immunogenic interaction of vaccine components with a host’s genetic programming. As all human physiology and constitution is underwritten by an individual’s genetic complement, it follows that unusual changes to health after vaccination are much more than just metabolic hiccups - they are genetic impairments that dysregulate primary cellular and molecular processes which are needed to ‘run’ the body.
Gherardi (2003, 162) referred to this immunogenic dysregulation as an unnatural and persistent immune activation that fails to switch off, that has pathological effects upon human physiology resulting in autoimmune diseases. Research by Gherardi and co-workers alerted to the aluminium adjuvants used in vaccines such as Hepatitis A and B, Tetanus and Anthrax vaccines; such adjuvants acting as potent immunostimulatory compounds upon the human immune system, and having the propensity to chronically shift an individual’s immune response leading to a cascade of adverse symptoms in genetically susceptible individuals. Aluminium hydroxide was the adjuvant used in the vaccine the author received.
Hamza et.al. (2012, 516) provided further clarification for these immune shifts, by describing one of the intrinsic mechanisms that falters after vaccination takes place. Using in vitro and mouse liver models, Hamza et. al. found “that the hepatitis B vaccine exposure resulted in significant upregulation (ie: an unscheduled encoding) of .. key genes….” and their regulatory caspase/kinase complexes, involving the intrinsic apoptotic pathway. They concluded “that exposure of Hepa 1-6 (liver) cells to a low dose of adjuvanted hepatitis B vaccine leads to loss of mitochondrial integrity, apoptosis induction, and cell death….” In layman’s terms, the aluminium hydroxide added to HBV’s induces a rapid and premature cell suicide on a massive scale - an apoptotic suicide of healthy functioning liver cells (as in the author’s injury). The impact of this heavy metal stimulant is probably augmented by the peculiar genetically modified viral genome in the vaccine, also suspected of triggering cytotoxicity via genetic dysregulation.
Interestingly – but unfortunately, the author began to experience digestive and bowel disturbances soon after the onset of injury. These disturbances were typical of Irritable Bowel Syndrome (IBS) and included abdominal bloating and pain, intestinal churning sensation, foamy urine, loose frothy and pale stools, food poisoning events, and food intolerances to gluten, certain canned foods and oral penicillin antibiotics. The sudden onset of IBS was no doubt related to immunogenic damage from vaccine upregulation or degradation. Whether this damage occurred via the enteric nervous system, or via the gut-brain axis, or the liver pathway, or the intestinal barrier pathway, or the microbiota synergism pathway (dysbiosis), or from a combination of these; is presently undefined.
The link between liver disorders and IBS has been a subject of investigation by various researchers. In their review of this literature Scalera et. al. (2013) proposed the question: “Can metabolic liver disease affect the functions of the gastrointestinal tract leading to syndromic manifestations typical of IBS…..?” In their search for a link between IBS and fatty/inflammatory liver states they concluded: “The above-mentioned evidence suggests that innate immunity is a main pathogenetic component of both NAFLD (non-alcoholic fatty liver disease) and IBS…..Although the disease (IBS) has not been overtly related to an inflammatory systemic disease, IBS is characterized by hyper-activation of the immune system and general inflammation…..NAFLD and IBS are classically defined as different diseases……But, surprisingly, there are many points of contact …… which are fundamental to their pathogenesis, being related to the immune activation and inflammation.”
The unnatural and persistent immune activation that fails to switch off, that has pathological effects upon human physiology, that Gherardi (2003, 162) and Hamza et. al. (2012, 516) attributed to aluminium hydroxide components of vaccines; is one such mechanism of injury for the author’s liver and GIT pathogenesis. The combination of this metallic oxide mechanism with the viral genome mechanism probably accounts for the exponential autoimmune disturbances frequently exhibited in injured recipients. The peculiar human genetic sensitivity associated with the hepatitis B viral genome, is discussed later in Part 3 under ‘Lymphocyte Subsets’.
Ø Part 3. BODY FLUID PATHOLOGIES:
The serum, urine and faecal test data compiled in Tables 2 & 3 demonstrate that a significant immunological upheaval occurred in the author’s health after receiving two HBV inoculations. The tabulated data provides chemical and genetic evidence of modes of injury, thus producing a clinical picture of the internal disruption the vaccine initiated upon the author’s health. The hepatic, lymphatic and neuromuscular systems were the first to become inflamed or impaired, followed by the digestive system. The collation of important immune markers from this data, are illustrated in the Serology Timeline graphs below. (See also the PDF style hand drawn graphs attached).
Subdivisions: (Findings from Tables 2, 3):
- Liver Enzyme Disruption 41
- Pathogenic Sensitivity Screening 43
- ESR/CRP/UMC/FB Non-specific Screening 45
- Pre-existing Conditions Screening 47
- Total White Blood Cell Count Reactivity 48
- White Blood subsets: Neutrophils and Lymphocytes 51
- Lymphocyte Subsets: Autoimmune Dysregulation 54
· Figures 1- 4: Serology timeline graphs.
· Table 4: ESR, CRP, UMC, Faecal screening results
· Table 5: Persisting cytotoxic subsets (NK and T cells)
· Table 6: Potential markers for CFS activation
· Table 7: Common MS symptoms correlation
· Table 8: Affected body systems & symptoms
LIVER ENZYME DISRUPTION - Fig 1: (Findings from Table 2):
The disruption to the author’s health was particularly evident in the changes to liver enzyme levels, and corresponds to the hepatic swelling demonstrated in the previous discussion on ultrasound findings. The swelling (hepatitis) and enzyme changes of the liver also correlate with “serious events” declared by HBV manufacturers, who document side-effects such as “abnormal LFT’s”, “changes to LFT’s”, or “tissue swelling”.
The data shows alkaline phosphatase (ALP) at first dropped after the 2nd inoculation, then rose (ie: 60 > 55 > 73), then steadily climbed to 93 U/L over a 2 year period. Another 1.5 years passed before this enzyme settled to the control value on 17.06.13. ALT enzyme levels tripled from 41 to 124 U/L in the first 3 months (a massive increase), and remained erratic for 2.25 years before settling. AST enzyme levels rose from 32 to 51 U/L before dropping, but remained erratic for 3 years. Kidney function showed no obvious disruption, with creatinine and electrolyte levels remaining within normal range parameters. The enzyme disruptions are illustrated in Figure 1 below.
This Section is divided into the following parts:
Ø Part 1: NEUROLOGY PATHOLOGIES:
- NCV findings
Ø Part 2: IMAGING PATHOLOGIES:
- Ultrasound findings
- CT Scan findings
- MRI Scan findings
Ø Part 3: BODY FLUID PATHOLOGIES:
- Liver Enzyme Disruption
- Pathogenic Sensitivity Screening
- ESR/CRP/UMC/FB Non-specific Screening
- Pre-existing Conditions Screening - Total White Blood Cell Count Reactivity
- White Blood subsets: Neutrophils and Lymphocytes
- Lymphocyte Subsets: Autoimmune Dysregulation
Ø Part 4: OVERVIEW AT THE 5 YEAR MARKER.
Ø Part 1. NEUROLOGY PATHOLOGIES:
- NCV findings:
The human nervous system may be divided into the Central, Enteric, Peripheral, and Autonomic nervous systems. Injury to either system may result in a variety of symptoms to limbs, abdomen, or the head. If such injury arises, the services of a neurologist may be required to investigate the source and extent of any nerve damage. Many neurologists have reportedly shown reluctance in undertaking investigations for vaccine victims. To document vaccine damage could invite scorn from one’s peers and jeopardy to one’s career, as some health agencies regard this help as dissent.
A condition of low grade paralysis had occurred in the author’s legs in the first three months of illness (the acute phase), where mobility was limited to about 10 steps to the toilet and return to bed. The legs were acutely weakened and woody. After the bed confinement had passed, the legs remained in a state of chronic weakness requiring a mobility frame for shopping excursions. Subsequent research revealed that leg disorders were a common symptom in the testimonies of vaccine injured victims.
Accordingly, a neurologist was consulted to investigate the author’s mobility problems. Despite a number of neurological tests being available, the neurologist undertook only one test, that being a Nerve Conduction Velocity test (NCV). This simple electrical test measures straight line conductivity of electrical impulses as they are transmitted along nerve bundles, primarily from point A to point B. Decreases in the velocity of impulses at normal body temperatures, may indicate nerve disease or injury to muscle function. NCV tests help identify conditions such as Guillaine-barre syndrome, carpal tunnel, Charcot-Marie tooth disease, herniated disc disease, chronic inflammatory polyneuropathy and neuropathy, sciatic nerve complaints, pinched or crushed nerves, and Peripheral injuries including numbness and tingling or itching.
The NCV test was undertaken on the 08 April 2010, about one year after the onset of illness, during the Intermediate phase of the injury. The test was performed on the legs while at rest in the seated position. There were no conduction irregularities cited by the neurologist from this test at that time. No further neurological tests have been followed up or recommended by the neurologist, despite persisting leg weakness.
The potential deficiency in the NCV test was that conduction was measured only between two points primarily along a major nerve bundle, without reference to the capacities of numerous lateral nerve synapses. The deficiency of the NCV test undertaken becomes apparent in that it does not measure ‘strain’ (or load). It does not measure the leg weakness the author feels first thing out of bed, or the strain after walking short distances of 50 to 75 m using a wheelie walker. It also does not measure the particular ‘woodiness’ the author has felt when prompted to skip a few metres to avoid an oncoming vehicle, whereas prior to vaccination the legs could run swiftly and fluidly without any impedance. These are loads not measured by the NCV test.
The fact that involuntary muscle tremors were experienced for 2 years reducing to episodic spasms, and that chronic weakening of the legs occurred requiring a mobility frame, strongly suggests the onset of a neuromuscular disorder following vaccination.
Ø Part 2. IMAGING PATHOLOGIES:
- Ultrasound findings
- CT Scan and MRI Scan findings
Chronology: 1st Ultrasound - 02. 06. 2009 Abdomen.
2nd Ultrasound - 30. 09. 2009 Abdomen.
1st CT Scan - 08. 01. 2010 Lumbar Spine.
1st MRI Scan - 11. 10. 2010 Abdomen.
3rd Ultrasound - 01. 09. 2011 Abdomen.
4th Ultrasound - 01. 02. 2012 Scrotum.
The 1st Ultrasound results found that: “The liver shows moderate fatty changes as well as enlargement of the left lobe and the caudate lobe” (02.06. 2009). The occurrence of this sudden and acute liver inflammation (ie: a hepatitis condition) for several months after the 2nd inoculation, was one of the early pieces of evidence that demonstrated that a significant injury was in progress, for which there were no contributing lifestyle factors (ie: no fatty diets, no fast foods, no alcoholic habits, no lethargic habits, and no identifiable pathogens). This first abdominal investigation was performed some 12 weeks after the 2nd inoculation, when the author was 50 years old. The findings of this ultrasound supports the proposition for this study that the vaccine solely caused the author’s injury, including the liver inflammation noted here.
The 2nd Ultrasound undertaken on 30.09.09, a further 12 weeks after the first ultrasound, found no visible liver abnormality remaining. The withdrawal of the swelling and fatty condition after the acute phase ended, further implicates vaccine causality for this transient hepatitis, rather than the condition being virally activated. Liver viremias are typified by persisting fatty infiltration which may be chronic for some years after infection passes. The fattiness of the author’s liver did not persist, indicating non-pathogenic disruption to liver histology.
The 1st MRI also showed that the visible structural injury to the liver was no longer visible despite continuing abdominal pain in the liver region. The MRI did not detect any lesions or cirrhosis of the liver, indicating that no chronic hepatic trauma had ever been sustained to the liver before vaccination (such as the effects of substance abuses). In other words, the author’s liver was in excellent condition before the post- vaccination “enlargement” occurred.
The 3rd Ultrasound gave the same results as the 2nd, indicating no abnormalities at the focal / structural plane, and no reversion back to acute phase pathologies. The 4th Ultrasound detected no focal abnormalities to the testes, the scrotal pain most likely representing diffuse myalgia often associated with post-vaccination pathologically induced neuromuscular disorder.
The CT Scan of the lower back demonstrated no disc protrusions, no nerve entrapments, and no vertebral compression at any level, indicating no spinal inflammatory hereditary conditions. There was detected only mild degenerative change between 3 vertebrae, indicating the normal effects of physical labour over time in combination with deterioration associated with aging. The back pain which prompted this test may have been an artifact of the Acute and Intermediate phase symptoms, as the author did not usually suffer from persisting back pain before vaccination.
Thus, as noted above, the primary injury visible from the imaging tests was to the liver. The 1st Ultrasound confirmed that a structural injury occurred to the liver soon after vaccination, namely swelling and fatty reactions, which remained for a limited period of some 3-5 months. The 2nd Ultrasound concluded that the swelling and fattiness had subsided. Serology confirmed that disruption to the liver was of non-pathogenic origin. Serology also confirmed that large amounts of liver enzymes were released into the bloodstream at the time of the enlargement, and that those releases remained abnormally high or erratic before settling about 3 to 3.5 years after the inoculations were given (see next section). The liver reaction is therefore best described as a Toxic Hepatitis, a condition known to occur as a result of the adverse impression certain drugs create upon human physiology – in this case the vaccine.
Regulated serum release of liver enzymes within normal range parameters, is part of the normal maintenance process of non-inflammatory gradual cell death (apoptosis) and cell replacement. However, large enzyme releases into the bloodstream, as is noted in the author’s test results, are typically a sign of inflammatory and premature cell death of hepatocytes (liver cells). In other words, an apoptotic cascade occurred following vaccination, explaining why inflammation of the liver lobes became visible to the ultrasound. This enlargement signifies that a sudden cascade of cell death of massive proportions took place over several months, for which no pathogen could be identified. Inflammation is the primary source of pain and discomfort, and accounts for the RHS abdominal pain associated with this injury.
Despite the eventual subsidence of the enzymes after 3+ years, and the lack of any bile duct obstructions in subsequent scans, daily RHS abdominal pain has persisted to the 5 year marker indicating that long term injury to the liver has probably occurred. Lipski (2012, 20, 237) noted that the liver can lose as much as 70% of its capability and not show diagnosable data indicating liver disease, and that if the immune system attacks the liver, it is probably due to a genetic defect.
That ‘defect’ has been the subject of much scholarly investigation and in the case of vaccine-induced injury states, represents a chemically induced defect caused by the immunogenic interaction of vaccine components with a host’s genetic programming. As all human physiology and constitution is underwritten by an individual’s genetic complement, it follows that unusual changes to health after vaccination are much more than just metabolic hiccups - they are genetic impairments that dysregulate primary cellular and molecular processes which are needed to ‘run’ the body.
Gherardi (2003, 162) referred to this immunogenic dysregulation as an unnatural and persistent immune activation that fails to switch off, that has pathological effects upon human physiology resulting in autoimmune diseases. Research by Gherardi and co-workers alerted to the aluminium adjuvants used in vaccines such as Hepatitis A and B, Tetanus and Anthrax vaccines; such adjuvants acting as potent immunostimulatory compounds upon the human immune system, and having the propensity to chronically shift an individual’s immune response leading to a cascade of adverse symptoms in genetically susceptible individuals. Aluminium hydroxide was the adjuvant used in the vaccine the author received.
Hamza et.al. (2012, 516) provided further clarification for these immune shifts, by describing one of the intrinsic mechanisms that falters after vaccination takes place. Using in vitro and mouse liver models, Hamza et. al. found “that the hepatitis B vaccine exposure resulted in significant upregulation (ie: an unscheduled encoding) of .. key genes….” and their regulatory caspase/kinase complexes, involving the intrinsic apoptotic pathway. They concluded “that exposure of Hepa 1-6 (liver) cells to a low dose of adjuvanted hepatitis B vaccine leads to loss of mitochondrial integrity, apoptosis induction, and cell death….” In layman’s terms, the aluminium hydroxide added to HBV’s induces a rapid and premature cell suicide on a massive scale - an apoptotic suicide of healthy functioning liver cells (as in the author’s injury). The impact of this heavy metal stimulant is probably augmented by the peculiar genetically modified viral genome in the vaccine, also suspected of triggering cytotoxicity via genetic dysregulation.
Interestingly – but unfortunately, the author began to experience digestive and bowel disturbances soon after the onset of injury. These disturbances were typical of Irritable Bowel Syndrome (IBS) and included abdominal bloating and pain, intestinal churning sensation, foamy urine, loose frothy and pale stools, food poisoning events, and food intolerances to gluten, certain canned foods and oral penicillin antibiotics. The sudden onset of IBS was no doubt related to immunogenic damage from vaccine upregulation or degradation. Whether this damage occurred via the enteric nervous system, or via the gut-brain axis, or the liver pathway, or the intestinal barrier pathway, or the microbiota synergism pathway (dysbiosis), or from a combination of these; is presently undefined.
The link between liver disorders and IBS has been a subject of investigation by various researchers. In their review of this literature Scalera et. al. (2013) proposed the question: “Can metabolic liver disease affect the functions of the gastrointestinal tract leading to syndromic manifestations typical of IBS…..?” In their search for a link between IBS and fatty/inflammatory liver states they concluded: “The above-mentioned evidence suggests that innate immunity is a main pathogenetic component of both NAFLD (non-alcoholic fatty liver disease) and IBS…..Although the disease (IBS) has not been overtly related to an inflammatory systemic disease, IBS is characterized by hyper-activation of the immune system and general inflammation…..NAFLD and IBS are classically defined as different diseases……But, surprisingly, there are many points of contact …… which are fundamental to their pathogenesis, being related to the immune activation and inflammation.”
The unnatural and persistent immune activation that fails to switch off, that has pathological effects upon human physiology, that Gherardi (2003, 162) and Hamza et. al. (2012, 516) attributed to aluminium hydroxide components of vaccines; is one such mechanism of injury for the author’s liver and GIT pathogenesis. The combination of this metallic oxide mechanism with the viral genome mechanism probably accounts for the exponential autoimmune disturbances frequently exhibited in injured recipients. The peculiar human genetic sensitivity associated with the hepatitis B viral genome, is discussed later in Part 3 under ‘Lymphocyte Subsets’.
Ø Part 3. BODY FLUID PATHOLOGIES:
The serum, urine and faecal test data compiled in Tables 2 & 3 demonstrate that a significant immunological upheaval occurred in the author’s health after receiving two HBV inoculations. The tabulated data provides chemical and genetic evidence of modes of injury, thus producing a clinical picture of the internal disruption the vaccine initiated upon the author’s health. The hepatic, lymphatic and neuromuscular systems were the first to become inflamed or impaired, followed by the digestive system. The collation of important immune markers from this data, are illustrated in the Serology Timeline graphs below. (See also the PDF style hand drawn graphs attached).
Subdivisions: (Findings from Tables 2, 3):
- Liver Enzyme Disruption 41
- Pathogenic Sensitivity Screening 43
- ESR/CRP/UMC/FB Non-specific Screening 45
- Pre-existing Conditions Screening 47
- Total White Blood Cell Count Reactivity 48
- White Blood subsets: Neutrophils and Lymphocytes 51
- Lymphocyte Subsets: Autoimmune Dysregulation 54
· Figures 1- 4: Serology timeline graphs.
· Table 4: ESR, CRP, UMC, Faecal screening results
· Table 5: Persisting cytotoxic subsets (NK and T cells)
· Table 6: Potential markers for CFS activation
· Table 7: Common MS symptoms correlation
· Table 8: Affected body systems & symptoms
LIVER ENZYME DISRUPTION - Fig 1: (Findings from Table 2):
The disruption to the author’s health was particularly evident in the changes to liver enzyme levels, and corresponds to the hepatic swelling demonstrated in the previous discussion on ultrasound findings. The swelling (hepatitis) and enzyme changes of the liver also correlate with “serious events” declared by HBV manufacturers, who document side-effects such as “abnormal LFT’s”, “changes to LFT’s”, or “tissue swelling”.
The data shows alkaline phosphatase (ALP) at first dropped after the 2nd inoculation, then rose (ie: 60 > 55 > 73), then steadily climbed to 93 U/L over a 2 year period. Another 1.5 years passed before this enzyme settled to the control value on 17.06.13. ALT enzyme levels tripled from 41 to 124 U/L in the first 3 months (a massive increase), and remained erratic for 2.25 years before settling. AST enzyme levels rose from 32 to 51 U/L before dropping, but remained erratic for 3 years. Kidney function showed no obvious disruption, with creatinine and electrolyte levels remaining within normal range parameters. The enzyme disruptions are illustrated in Figure 1 below.
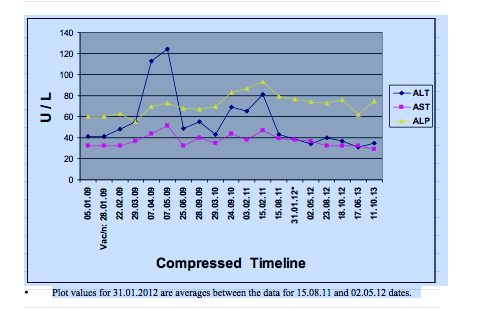
Figure 1: Changes in liver enzymes in Paul Taggert following HBV inoculations.
The analysis of the liver pathologies demonstrates:
o There was no inherent fatty liver condition shown by a return to normal histology.
o ALP enzyme in 2004 was 60 U/L, historically mirroring the 01.05.09 Control.
o There were no other liver conditions therefore, from past substance abuse.
o The new changes to liver chemistry and histology, thus presents a picture of drug induced damage to hepatocytes within a predictable immunological timeframe.
o The persisting RHS abdominal pain 5 years after inoculation, demonstrates chronic trauma to the liver, rendering it weakened or ‘tender’.
o The pathology findings strongly support the manufacturer’s stated side-effects.
PATHOGENIC SENSITIVITY SCREENING : (Tables 3 Findings):
Abbreviations:
Cytomegalovirus (CMV)
Epstein Barr Virus (EBV)
Infectious Mononucleosis (IM)
Toxoplasma gondii – (Toxoplasmosis)
Immunoglobulin M – (IgM): short term antibodies indicator for acute phase pathogen.
Immunoglobulin G – (IgG): long term antibodies indicator for chronic/past exposure.
Table 1 summarizes the regimen of tests undertaken to identify or exclude pathogenic causes including tests for mosquito pathogens, hepatitis pathogens, STD pathogens, and miscellaneous pathogens. Despite the debilitating illness the author endures following vaccination, not a single disease of contemporary occurrence could be identified or associated with the author’s clinical picture.
All of the diseases tested for and described in Table 3 returned negative results except for two past exposures, being CMV and Toxoplasma. These two pathogens are shown by the serology to be old exposures, with immunoglobulin antibody indicators confirming that both pathogens had no involvement in the current injury whatsoever. EBV was also tested for twice after the injury onset (on 7 May and 25 June 2009), both tests returning negative exposure for acute (IgM) and chronic (IgG) capsid and nuclear antigens. All Q Fever tests returned negative IgM indicators while IgG indicators returned an equivocal response, providing no confirmable past exposure. An equivocal response is a ‘nothing’ response from which no conclusions can be drawn, and may in fact be a repeating biological false-positive result.
CMV, Toxoplasmosis, and EBV share a common feature – they infect many people without any symptoms felt (known as asymptomatic infections). Such silent exposures apply to many other diseases in various regions of the world. They are called silent diseases because they pass through unnoticed in large numbers of people, (unlike cold and flu viruses which usually have observable symptoms). Lanari et. al. (2006) noted: “Human cytomegalovirus (CMV) is a ubiquitous human-specific DNA virus that belongs to the Herpesviridae family. More than 90% of primary infections are asymptomatic in healthy adults and children…..” CMV and EBV are responsible for the self-limiting condition medically identified as Infectious Mononucleosis (IM). Both viruses occur mostly in silent form in childhood to adolescence, or on occasions when in observable form, are limited to transient flu-like symptoms or glandular fever that pass after a couple of weeks. Their ubiquitous occurrence in humans suggests a long evolutionary association in human immune development and maturation.
Given the asymptomatic nature of many infections, a ‘Positive’ exposure to any pathogen (written on any laboratory print-out), is therefore not a confirmation that any adverse symptoms accompanied that past exposure. Similarly, the author’s exposure to CMV and Toxoplasma is likely to have been typically asymptomatic. Furthermore, the serology does not show any acute IgM antibodies contemporary with the present injury, confirming that the primary infections for these two pathogens occurred before the last ten years and more probably many years before the timeframe of this report.
Importantly, the author’s clinical picture and empirical evidence demonstrates that full suppression of CMV and Toxoplasma pathogenesis had been effectively maintained during the entire acute/intermediate phases of injury following vaccination, evidenced by the lack of any elevation of IgG immunoglobulins in the tests performed for these two pathogens during Feb-May 2009. Thus, any reactivation or recurrence of chronic CMV or Toxoplasma antibodies cannot be demonstrated in the serology. Riddell et. al. (1991) noted the following remarks about CMV suppression:
“CMV is a common human pathogen that acutely infects more than 50% of the normal population, but generally causes only minor symptoms. After initial exposure, the virus is carried lifelong in healthy individuals as a latent or persistent infection without any apparent clinical syndrome…. The data demonstrate that the major CTL response to CMV can recognise and lyse infected target cells before the expression of any viral genes, and suggests that such a response may have a biologically important role in controlling latent or persistent CMV infection.”
As CMV, EBV and Toxoplasmosis are self limiting diseases that have no latent symptoms in healthy individuals with unsuppressed immune systems, any claim that past exposures suddenly reactivated coincidentally soon after vaccination, would be medically irresponsible. The serology demonstrates that:
o no adverse symptoms have ever been confirmed from any of the four pathogens
o no flare-up of reactivated IgG antibodies could be identified after vaccination
o no pathogenic activity could be identified whatsoever from CRP, ESR, UMC tests
o no evidence of immunosuppression or compromise exists before vaccination
o therefore no clinical picture exists to support any recurrence of either pathogens
o to make similar claims for the Q Fever test anomaly would be equally wrong.
The test results for Hepatitis viral infection in Table 3 are also significant. Although the ultrasound tests confirmed a hepatitis condition occurred soon after vaccination, the classical symptoms of acute phase jaundice and rusty-coloured urine were absent. Also, there were no Ig/M or Ig/G antibodies identified in the serology to the Hepatitis A,B,C, viruses, further demonstrating no infection occurred from a live Hepatitis virus pathogen at any time before vaccination.
The absence of active concurrent pathogenic markers throughout the serology, strongly implicates the Hepatitis B vaccine as the sole causal agent of injury, which induced significant LFT changes and sudden swelling of the liver tissues, ie: a non-pathogenic chemical hepatitis. This Toxic Hepatitis of the liver identified by the 1st Ultrasound, also correlates with the adverse reports declared by HBV manufacturers, whose package inserts acknowledge: ‘abnormal LFT’s”, and “tissue swelling” as known side-effects.
ESR / CRP / UMC RANDOM NON-SPECIFIC SCREENING: (Tab 4):
Abbreviations:
Erythrocyte Sedimentation Rate (ESR)
C-Reactive Protein (CRP)
Urine Micro Culture (UMC)
Faecal Bioassay (FB)
ESR, CRP, and UMC are broad spectrum non-specific laboratory tests used to identify the presence of pathogenic activity in the body. These tests were undertaken on multiple occasions over the 4.5 year investigation period, their results being included in Table 3. For convenience, these same results have been lifted and collated into Table 4, below.
ESR and CRP are both haematology markers used to screen for non-specific sources of inflammation or pathogenic infection. The tests are frequently and commonly used in the medical industry. Both tests have clinical limitations, in that neither is able to identify specific causes of infection or sources of inflammation. Both tests also do not possess a 100% detection rate, meaning that a person can be very ill but show no ESR or CRP increases at all, although this may not be usual. These tests can indicate however, that irregular or foreign processes are occurring somewhere in the body. The rule of thumb for these two tests is, ‘If detection registers during testing, then the higher the value – the more active is the disorder or more serious is the infection’.
ESR tests measure the rate of separation of red blood cells (erythrocytes) from plasma. Normal ESR values vary from lab to lab. The normal range for this study is from 0 - 20 mm / hr for middle aged males. Increased levels represent markers for various cancers, muscular and connective tissue disorders, autoimmune diseases, organ diseases, or bacterial infections. All five ESR tests listed in Table 4 registered no pathogenic activity across the period of injury.
CRP is an acute-phase pentraxin protein produced by the liver when there is infection or inflammation in the body. Changes in the CRP are more rapid than changes in the ESR. Normal CRP values vary from lab to lab. The normal health range for this study is 0 - 6 mg / L., (although some labs may choose an upper limit of 10 mg). Low levels do not always indicate an absence of inflammation or infection. Developed in 1930, CRP is a useful non-specific identifier of a range of clinically significant and systemic inflammatory disorders (cancers, rheumatoid, autoimmune, bone and bowel disorders), and is also a useful general marker for alerting diagnosticians to the presence of bacterial, viral, and fungal infections. All seven CRP tests tabulated registered no pathogenic activity across the period of injury.
UMC is another laboratory test used to analyse bladder urine in order to determine the presence or absence of bacteria or fungi in the urinary tract. If left untreated, urinary tract infections (UTI’s) can spread to other areas of the body. UMC tests require 2-3 days for pathogens (if any) to multiply in urine culture, before a lab result can be finalized. All six UMC tests tabulated, registered no pathogenic activity across the period of injury.
Table 4. Screening results for random pathogenic reactivity, condensed from Table 3:
.
Date Test Name Results Comments .
05.01.09 Erythrocyte Sed. Rate 8 mm / hr Normal
07.04.09 Erythrocyte Sed. Rate 5 mm / hr Normal
07.05.09 Erythrocyte Sed. Rate 5 mm / hr Normal
24.09.10 Erythrocyte Sed. Rate 5 mm / hr Normal
02.05.12 Erythrocyte Sed. Rate 5 mm / hr Normal
22.02.09 C Reactive Protein 1.6 mg / L Normal
07.04.09 C Reactive Protein < 5 mg / L Normal
07.05.09 C Reactive Protein < 5 mg / L Normal
29.03.10 C Reactive Protein < 5 mg / L Normal
31.01.12 C Reactive Protein < 2 mg / L Normal
17.06.13 C Reactive Protein < 0.7 mg / L Normal
11.10.13 C Reactive Protein < 0.7 mg / L Normal
27.02.09 Urine Micro Culture <10 No growth Normal
07.04.09 Urine Micro Culture <10 No growth Normal
07.05.09 Urine Micro Culture <10 No growth Normal
06.07.09 Urine Micro Culture <10 No growth Normal
29.03.10 Urine Micro Culture <10 No growth Normal
17.06.13 Urine Micro Culture <10 No growth Normal
07.04.09 Faeces OCP & M/C/S Some cysts No pathogens
16.10.09 Faeces OCP & M/C/S Some microbes No pathogens
06.11.09 Faeces OCP & M/C/S No parasites No pathogens
29.03.10 Faeces M/C/S No parasites No pathogens
.
Finally, the four faecal tests (FB) found microbial evidence of Dientamoeba fragilis and cysts of Blastocystis hominis, but culturing these samples isolated no bacterial pathogens. As there were no reportable bowel problems in the years before vaccination, the cysts may represent the past ingestion of microbes from town water supplies or raw food consumption. The GIT is a milieu inhabited by billions of microbes. The presence of Dientamoeba and Blastocystis microbes at one time does not provide any evidence of damage to the host. It is more likely they co-existed in the GIT in symbiotic or harmless cohabitation. Such an asymptomatic association is not uncommon in many societies, and their significance should not be exaggerated.
Through all of these non-specific tests, one common denominator stands out – there was no bacterial pathogenesis detectable by these tests in the author’s samples. The combination of these broad spectrum non-specific tests with the testing regimen for specific sensitivity pathogens, together supports the proposition at the beginning of this section, that there were no pathogens of any kind, either past or contemporary to the injury, which could be found responsible for causing the author’s sudden and devastating injury. Thus, a refined exclusion diagnosis of ‘Non-Pathogenic Causality’ is supported by these investigations.
PRE-EXISTING CONDITIONS SCREENING: (Table 3):
A number of serology tests recorded in this study serve to identify the presence or absence of any pre-existing conditions in the author before 2009. These tests were undertaken mainly on the 05.01. 2009 just before vaccination, and contain data showing there were no pre-existing conditions involving any of the following:
o Thyroid – the test returned normal results (Euthyroid level), showing there were no systemic hormonal disorders related to the thyroid before inoculation. The thyroid is a major regulatory gland having broad influence over the body.
o Rheumatoid – the test returned normal results, showing there was no history of systemic disorders such as arthritis, dystrophy, myalgia, rheumatism, or synovitis. An orthopaedic assessment performed on 15.11.2011 for a separate physical work injury to the forearms (before vaccination), found there were no rheumatoid factors involved in that injury, which correlates precisely to the findings here.
Diabetes – Liver function tests (LFT’s) showed a normal glucose level of 5.2 (fasting) before inoculation, indicating no presence of glycaemic disorders. After o vaccination glucose levels increased mildly in Table 2, but promptly returned to the level 5’s indicating a further absence of diabetic disorders.
o Renal – LFT and UMC test results showed there were no pre-existing disorders relating to kidney function. Electrolyte, protein, glucose and ketones returned normal results before inoculation, indicating an absence of kidney disorders.
o Skeletal - The CT Scan of the lumbar spine on 08.01.2010, demonstrated no disc protrusions, no nerve entrapments, and no vertebral compression at any level, indicating no osteopathic tendencies before or after vaccination.
o Oncological – Two tests were performed on 15.08.11 and 17.06.13 to detect the presence of prostrate cancer. Both tests returned normal results.
o Autoimmune – An Antinuclear Antibody Test (ANA), returned negative results. A negative result usually excludes active Systemic Lupus Erythematosus (SLE), a disease where the immune system attacks the body’s own connective tissues.
o Microbial Pathogens – no active pathogenesis detectable, as previously discussed.
o Coeliac – Dermal allergy testing for wheat, rye and oats in November 2000, found no reactions to the skin after exposure to concentrates of these grains. There was no regular intolerance to wheaten foods before inoculation. After vaccination the author suffered from gluten-like reactions. Only rolled oats were tolerable due to their low gluten content. On the 29.03.10 a Coeliac Master test was performed which returned normal results indicating no hereditary allergy to gluten, but threshold reactions indicate post-vaccination non-coeliac gluten-like intolerance.
o Lipids – total serum cholesterol before and after vaccination has averaged about 3.8 mmol/L, indicating no hepatic tendencies relating to fatty disorders.
TOTAL WHITE BLOOD CELL COUNT REACTIVITY: ( Table 2):
In the previous sections, serology findings concluded that pathogens and pre-existing conditions were not involved in the development of the author’s injury. However, serology showed significant liver enzyme releases in conjunction with liver swelling, which now directs this investigation towards the analysis of other blood irregularities.
Beginning with Table 2 data, the pre-vaccination test dated 5.1.09 shows the author’s normal and routine WCC serum range. This test serves as the “control” previously noted. The second plot value (only) of 5.0 is an estimate (just before inoculation), based upon the author’s average WCC history. Soon after inoculation the WCC rapidly increased from 5.0 to 8.9, ie: nearly double the control level, and approaching the medical condition known as Leukocytosis. This unusual increase is illustrated in Figures 2(a) and 2(b) below.
Note the sudden and massive WCC increase in both graphs following the point of inoculation on 28.01.2009. Judging by the angle of increase visible in the plot lines of both graphs, the WCC may have peaked at c.9.5, but the two subsequent serum tests (07.05.09 and 25.06.09) gave no data to confirm this, despite LFT’s being performed for both these dates. However, the LFT for the 07.05.09 showed enzyme levels continued to increase past the previous test date (07.04.09), so it is safe to assume that the WCC also showed the same tendency to rise. Thus, WCC must have passed 9.0 for a short period.
The analysis of the liver pathologies demonstrates:
o There was no inherent fatty liver condition shown by a return to normal histology.
o ALP enzyme in 2004 was 60 U/L, historically mirroring the 01.05.09 Control.
o There were no other liver conditions therefore, from past substance abuse.
o The new changes to liver chemistry and histology, thus presents a picture of drug induced damage to hepatocytes within a predictable immunological timeframe.
o The persisting RHS abdominal pain 5 years after inoculation, demonstrates chronic trauma to the liver, rendering it weakened or ‘tender’.
o The pathology findings strongly support the manufacturer’s stated side-effects.
PATHOGENIC SENSITIVITY SCREENING : (Tables 3 Findings):
Abbreviations:
Cytomegalovirus (CMV)
Epstein Barr Virus (EBV)
Infectious Mononucleosis (IM)
Toxoplasma gondii – (Toxoplasmosis)
Immunoglobulin M – (IgM): short term antibodies indicator for acute phase pathogen.
Immunoglobulin G – (IgG): long term antibodies indicator for chronic/past exposure.
Table 1 summarizes the regimen of tests undertaken to identify or exclude pathogenic causes including tests for mosquito pathogens, hepatitis pathogens, STD pathogens, and miscellaneous pathogens. Despite the debilitating illness the author endures following vaccination, not a single disease of contemporary occurrence could be identified or associated with the author’s clinical picture.
All of the diseases tested for and described in Table 3 returned negative results except for two past exposures, being CMV and Toxoplasma. These two pathogens are shown by the serology to be old exposures, with immunoglobulin antibody indicators confirming that both pathogens had no involvement in the current injury whatsoever. EBV was also tested for twice after the injury onset (on 7 May and 25 June 2009), both tests returning negative exposure for acute (IgM) and chronic (IgG) capsid and nuclear antigens. All Q Fever tests returned negative IgM indicators while IgG indicators returned an equivocal response, providing no confirmable past exposure. An equivocal response is a ‘nothing’ response from which no conclusions can be drawn, and may in fact be a repeating biological false-positive result.
CMV, Toxoplasmosis, and EBV share a common feature – they infect many people without any symptoms felt (known as asymptomatic infections). Such silent exposures apply to many other diseases in various regions of the world. They are called silent diseases because they pass through unnoticed in large numbers of people, (unlike cold and flu viruses which usually have observable symptoms). Lanari et. al. (2006) noted: “Human cytomegalovirus (CMV) is a ubiquitous human-specific DNA virus that belongs to the Herpesviridae family. More than 90% of primary infections are asymptomatic in healthy adults and children…..” CMV and EBV are responsible for the self-limiting condition medically identified as Infectious Mononucleosis (IM). Both viruses occur mostly in silent form in childhood to adolescence, or on occasions when in observable form, are limited to transient flu-like symptoms or glandular fever that pass after a couple of weeks. Their ubiquitous occurrence in humans suggests a long evolutionary association in human immune development and maturation.
Given the asymptomatic nature of many infections, a ‘Positive’ exposure to any pathogen (written on any laboratory print-out), is therefore not a confirmation that any adverse symptoms accompanied that past exposure. Similarly, the author’s exposure to CMV and Toxoplasma is likely to have been typically asymptomatic. Furthermore, the serology does not show any acute IgM antibodies contemporary with the present injury, confirming that the primary infections for these two pathogens occurred before the last ten years and more probably many years before the timeframe of this report.
Importantly, the author’s clinical picture and empirical evidence demonstrates that full suppression of CMV and Toxoplasma pathogenesis had been effectively maintained during the entire acute/intermediate phases of injury following vaccination, evidenced by the lack of any elevation of IgG immunoglobulins in the tests performed for these two pathogens during Feb-May 2009. Thus, any reactivation or recurrence of chronic CMV or Toxoplasma antibodies cannot be demonstrated in the serology. Riddell et. al. (1991) noted the following remarks about CMV suppression:
“CMV is a common human pathogen that acutely infects more than 50% of the normal population, but generally causes only minor symptoms. After initial exposure, the virus is carried lifelong in healthy individuals as a latent or persistent infection without any apparent clinical syndrome…. The data demonstrate that the major CTL response to CMV can recognise and lyse infected target cells before the expression of any viral genes, and suggests that such a response may have a biologically important role in controlling latent or persistent CMV infection.”
As CMV, EBV and Toxoplasmosis are self limiting diseases that have no latent symptoms in healthy individuals with unsuppressed immune systems, any claim that past exposures suddenly reactivated coincidentally soon after vaccination, would be medically irresponsible. The serology demonstrates that:
o no adverse symptoms have ever been confirmed from any of the four pathogens
o no flare-up of reactivated IgG antibodies could be identified after vaccination
o no pathogenic activity could be identified whatsoever from CRP, ESR, UMC tests
o no evidence of immunosuppression or compromise exists before vaccination
o therefore no clinical picture exists to support any recurrence of either pathogens
o to make similar claims for the Q Fever test anomaly would be equally wrong.
The test results for Hepatitis viral infection in Table 3 are also significant. Although the ultrasound tests confirmed a hepatitis condition occurred soon after vaccination, the classical symptoms of acute phase jaundice and rusty-coloured urine were absent. Also, there were no Ig/M or Ig/G antibodies identified in the serology to the Hepatitis A,B,C, viruses, further demonstrating no infection occurred from a live Hepatitis virus pathogen at any time before vaccination.
The absence of active concurrent pathogenic markers throughout the serology, strongly implicates the Hepatitis B vaccine as the sole causal agent of injury, which induced significant LFT changes and sudden swelling of the liver tissues, ie: a non-pathogenic chemical hepatitis. This Toxic Hepatitis of the liver identified by the 1st Ultrasound, also correlates with the adverse reports declared by HBV manufacturers, whose package inserts acknowledge: ‘abnormal LFT’s”, and “tissue swelling” as known side-effects.
ESR / CRP / UMC RANDOM NON-SPECIFIC SCREENING: (Tab 4):
Abbreviations:
Erythrocyte Sedimentation Rate (ESR)
C-Reactive Protein (CRP)
Urine Micro Culture (UMC)
Faecal Bioassay (FB)
ESR, CRP, and UMC are broad spectrum non-specific laboratory tests used to identify the presence of pathogenic activity in the body. These tests were undertaken on multiple occasions over the 4.5 year investigation period, their results being included in Table 3. For convenience, these same results have been lifted and collated into Table 4, below.
ESR and CRP are both haematology markers used to screen for non-specific sources of inflammation or pathogenic infection. The tests are frequently and commonly used in the medical industry. Both tests have clinical limitations, in that neither is able to identify specific causes of infection or sources of inflammation. Both tests also do not possess a 100% detection rate, meaning that a person can be very ill but show no ESR or CRP increases at all, although this may not be usual. These tests can indicate however, that irregular or foreign processes are occurring somewhere in the body. The rule of thumb for these two tests is, ‘If detection registers during testing, then the higher the value – the more active is the disorder or more serious is the infection’.
ESR tests measure the rate of separation of red blood cells (erythrocytes) from plasma. Normal ESR values vary from lab to lab. The normal range for this study is from 0 - 20 mm / hr for middle aged males. Increased levels represent markers for various cancers, muscular and connective tissue disorders, autoimmune diseases, organ diseases, or bacterial infections. All five ESR tests listed in Table 4 registered no pathogenic activity across the period of injury.
CRP is an acute-phase pentraxin protein produced by the liver when there is infection or inflammation in the body. Changes in the CRP are more rapid than changes in the ESR. Normal CRP values vary from lab to lab. The normal health range for this study is 0 - 6 mg / L., (although some labs may choose an upper limit of 10 mg). Low levels do not always indicate an absence of inflammation or infection. Developed in 1930, CRP is a useful non-specific identifier of a range of clinically significant and systemic inflammatory disorders (cancers, rheumatoid, autoimmune, bone and bowel disorders), and is also a useful general marker for alerting diagnosticians to the presence of bacterial, viral, and fungal infections. All seven CRP tests tabulated registered no pathogenic activity across the period of injury.
UMC is another laboratory test used to analyse bladder urine in order to determine the presence or absence of bacteria or fungi in the urinary tract. If left untreated, urinary tract infections (UTI’s) can spread to other areas of the body. UMC tests require 2-3 days for pathogens (if any) to multiply in urine culture, before a lab result can be finalized. All six UMC tests tabulated, registered no pathogenic activity across the period of injury.
Table 4. Screening results for random pathogenic reactivity, condensed from Table 3:
.
Date Test Name Results Comments .
05.01.09 Erythrocyte Sed. Rate 8 mm / hr Normal
07.04.09 Erythrocyte Sed. Rate 5 mm / hr Normal
07.05.09 Erythrocyte Sed. Rate 5 mm / hr Normal
24.09.10 Erythrocyte Sed. Rate 5 mm / hr Normal
02.05.12 Erythrocyte Sed. Rate 5 mm / hr Normal
22.02.09 C Reactive Protein 1.6 mg / L Normal
07.04.09 C Reactive Protein < 5 mg / L Normal
07.05.09 C Reactive Protein < 5 mg / L Normal
29.03.10 C Reactive Protein < 5 mg / L Normal
31.01.12 C Reactive Protein < 2 mg / L Normal
17.06.13 C Reactive Protein < 0.7 mg / L Normal
11.10.13 C Reactive Protein < 0.7 mg / L Normal
27.02.09 Urine Micro Culture <10 No growth Normal
07.04.09 Urine Micro Culture <10 No growth Normal
07.05.09 Urine Micro Culture <10 No growth Normal
06.07.09 Urine Micro Culture <10 No growth Normal
29.03.10 Urine Micro Culture <10 No growth Normal
17.06.13 Urine Micro Culture <10 No growth Normal
07.04.09 Faeces OCP & M/C/S Some cysts No pathogens
16.10.09 Faeces OCP & M/C/S Some microbes No pathogens
06.11.09 Faeces OCP & M/C/S No parasites No pathogens
29.03.10 Faeces M/C/S No parasites No pathogens
.
Finally, the four faecal tests (FB) found microbial evidence of Dientamoeba fragilis and cysts of Blastocystis hominis, but culturing these samples isolated no bacterial pathogens. As there were no reportable bowel problems in the years before vaccination, the cysts may represent the past ingestion of microbes from town water supplies or raw food consumption. The GIT is a milieu inhabited by billions of microbes. The presence of Dientamoeba and Blastocystis microbes at one time does not provide any evidence of damage to the host. It is more likely they co-existed in the GIT in symbiotic or harmless cohabitation. Such an asymptomatic association is not uncommon in many societies, and their significance should not be exaggerated.
Through all of these non-specific tests, one common denominator stands out – there was no bacterial pathogenesis detectable by these tests in the author’s samples. The combination of these broad spectrum non-specific tests with the testing regimen for specific sensitivity pathogens, together supports the proposition at the beginning of this section, that there were no pathogens of any kind, either past or contemporary to the injury, which could be found responsible for causing the author’s sudden and devastating injury. Thus, a refined exclusion diagnosis of ‘Non-Pathogenic Causality’ is supported by these investigations.
PRE-EXISTING CONDITIONS SCREENING: (Table 3):
A number of serology tests recorded in this study serve to identify the presence or absence of any pre-existing conditions in the author before 2009. These tests were undertaken mainly on the 05.01. 2009 just before vaccination, and contain data showing there were no pre-existing conditions involving any of the following:
o Thyroid – the test returned normal results (Euthyroid level), showing there were no systemic hormonal disorders related to the thyroid before inoculation. The thyroid is a major regulatory gland having broad influence over the body.
o Rheumatoid – the test returned normal results, showing there was no history of systemic disorders such as arthritis, dystrophy, myalgia, rheumatism, or synovitis. An orthopaedic assessment performed on 15.11.2011 for a separate physical work injury to the forearms (before vaccination), found there were no rheumatoid factors involved in that injury, which correlates precisely to the findings here.
Diabetes – Liver function tests (LFT’s) showed a normal glucose level of 5.2 (fasting) before inoculation, indicating no presence of glycaemic disorders. After o vaccination glucose levels increased mildly in Table 2, but promptly returned to the level 5’s indicating a further absence of diabetic disorders.
o Renal – LFT and UMC test results showed there were no pre-existing disorders relating to kidney function. Electrolyte, protein, glucose and ketones returned normal results before inoculation, indicating an absence of kidney disorders.
o Skeletal - The CT Scan of the lumbar spine on 08.01.2010, demonstrated no disc protrusions, no nerve entrapments, and no vertebral compression at any level, indicating no osteopathic tendencies before or after vaccination.
o Oncological – Two tests were performed on 15.08.11 and 17.06.13 to detect the presence of prostrate cancer. Both tests returned normal results.
o Autoimmune – An Antinuclear Antibody Test (ANA), returned negative results. A negative result usually excludes active Systemic Lupus Erythematosus (SLE), a disease where the immune system attacks the body’s own connective tissues.
o Microbial Pathogens – no active pathogenesis detectable, as previously discussed.
o Coeliac – Dermal allergy testing for wheat, rye and oats in November 2000, found no reactions to the skin after exposure to concentrates of these grains. There was no regular intolerance to wheaten foods before inoculation. After vaccination the author suffered from gluten-like reactions. Only rolled oats were tolerable due to their low gluten content. On the 29.03.10 a Coeliac Master test was performed which returned normal results indicating no hereditary allergy to gluten, but threshold reactions indicate post-vaccination non-coeliac gluten-like intolerance.
o Lipids – total serum cholesterol before and after vaccination has averaged about 3.8 mmol/L, indicating no hepatic tendencies relating to fatty disorders.
TOTAL WHITE BLOOD CELL COUNT REACTIVITY: ( Table 2):
In the previous sections, serology findings concluded that pathogens and pre-existing conditions were not involved in the development of the author’s injury. However, serology showed significant liver enzyme releases in conjunction with liver swelling, which now directs this investigation towards the analysis of other blood irregularities.
Beginning with Table 2 data, the pre-vaccination test dated 5.1.09 shows the author’s normal and routine WCC serum range. This test serves as the “control” previously noted. The second plot value (only) of 5.0 is an estimate (just before inoculation), based upon the author’s average WCC history. Soon after inoculation the WCC rapidly increased from 5.0 to 8.9, ie: nearly double the control level, and approaching the medical condition known as Leukocytosis. This unusual increase is illustrated in Figures 2(a) and 2(b) below.
Note the sudden and massive WCC increase in both graphs following the point of inoculation on 28.01.2009. Judging by the angle of increase visible in the plot lines of both graphs, the WCC may have peaked at c.9.5, but the two subsequent serum tests (07.05.09 and 25.06.09) gave no data to confirm this, despite LFT’s being performed for both these dates. However, the LFT for the 07.05.09 showed enzyme levels continued to increase past the previous test date (07.04.09), so it is safe to assume that the WCC also showed the same tendency to rise. Thus, WCC must have passed 9.0 for a short period.
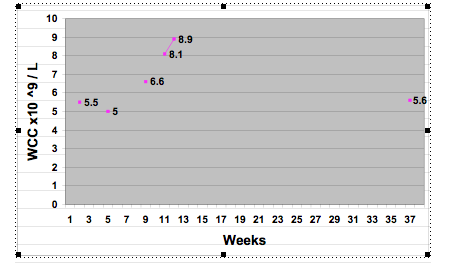
Figure 2 (a) : Chronological real-time progression of White blood Cell Count (WCC) in Paul Taggert following Hepatitis B vaccination.
The pathology provider gave no reason for the omission of WBC testing at these two crucial dates specified, despite the current increases warranting continual monitoring of WCC. WBC’s are used by the body to attack pathogens or contaminants, whether organic or synthetic. Their sudden increase in these test results demonstrates not only a sudden inflammatory shift in this important immune marker, but also a severe disruption to the rested immunity that the author previously exhibited.
Figure 2 (a): This first view of Figure 2 above shows only the first 37 weeks ( or 9 months) timeline in real-time scale, and shows the rise and fall of total WCC values. There are two gradient increases evident in the WCC values plotted in Figure 2(a). The meaning of a ‘gradient increase’ simply refers to the angle of increase visually present in the plot values from the adjacent horizontal. Figure 2(a) clearly shows a profound increase of 39 degrees in WCC plot values soon after the first inoculation, when applying a protractor to the printed graph. The delay between inoculation and the next serum increase (of 6.6) is three weeks. This increase did not stop there, but continued its pattern upwards to the next serum test which then showed a WCC of 8.1. In other words, this was no hiccup in WCC values due to a passing infection, but rather a demonstration of a serious threat to health from a foreign antagonist.
Three weeks before this second result of 8.1 was obtained, a second inoculation was received which produced the same three-week delayed increase (as the first inoculation), showing itself in the third serum test where the value had increased from 8.1 to 8.9 in only one week, representing a gradient increase of 59 degrees in the plot line, and a 20 degree (or 50%) increase in severity above the 1st reaction results. Total WCC values had thus increased about 80% above normal levels over 9.5 weeks.
The electronic graph generated herein for Figure 2(a) does display some visual limitation. The 2nd gradient increase is more clearly evident in the hand drawn (HD) graphs attached to this work , which are drawn to a larger format permitting greater accuracy down to 0.5 mm. The HD graph for Figure 2(a) is shown with the second WCC reading (for the 28th Jan) remaining at the same level of 5.5 as the control date (5th Jan), so that both pre-vaccination scenarios could be presented for this study, ie: where the WCC remained steady at 5.5 (in the HD graph), or, whether it (more probably) had dropped to c.5.0 immediately before inoculation (in the electronic graph). The difference here is academic. More importantly, the protractor readings from the HD graph, show a 1st gradient increase of 36 degrees, and a 2nd gradient increase of 52 degrees, and a difference in severity between both of 16 degrees. The second increase is visually more evident in the HD graph.
Thus in either format (electronic vss hand drawn), the 2nd gradient increase was more severe than the 1st gradient increase by 16 - 20 degrees, and both gradient increases occurred following exposure to the same drug (the vaccine). The 2nd, and greater gradient increase, therefore demonstrates an actual Positive Rechallenge event indicating the body’s stronger response to re-exposure to the same drug – measurable here in graphic presentation, and seen as the sharp increase from 8.1 to 8.9 in only 1 week.
A Positive Rechallenge is a recurrence of the same illness, with it’s symptoms and pathologies, but with a marked increase in severity or intensity, after the patient’s re-exposure to the same drug that caused the first reaction. This phenomenon is literally demonstrated above in Figure 2(a). Dr. Peter Fletcher, Chief Scientific Officer and Senior Principle Medical Officer of the UK’s Committee on Safety of Medicines (CSM), has stated: “The CSM has always accepted that positive rechallenge in the absence of other equivalent and credible causes has to be accepted as a causal relationship.” He further emphasized in the same paragraph, “the great importance of positive rechallenge cases which, for all practical purposes, prove causality.” (Wakefield 2011, i).
The pathology provider gave no reason for the omission of WBC testing at these two crucial dates specified, despite the current increases warranting continual monitoring of WCC. WBC’s are used by the body to attack pathogens or contaminants, whether organic or synthetic. Their sudden increase in these test results demonstrates not only a sudden inflammatory shift in this important immune marker, but also a severe disruption to the rested immunity that the author previously exhibited.
Figure 2 (a): This first view of Figure 2 above shows only the first 37 weeks ( or 9 months) timeline in real-time scale, and shows the rise and fall of total WCC values. There are two gradient increases evident in the WCC values plotted in Figure 2(a). The meaning of a ‘gradient increase’ simply refers to the angle of increase visually present in the plot values from the adjacent horizontal. Figure 2(a) clearly shows a profound increase of 39 degrees in WCC plot values soon after the first inoculation, when applying a protractor to the printed graph. The delay between inoculation and the next serum increase (of 6.6) is three weeks. This increase did not stop there, but continued its pattern upwards to the next serum test which then showed a WCC of 8.1. In other words, this was no hiccup in WCC values due to a passing infection, but rather a demonstration of a serious threat to health from a foreign antagonist.
Three weeks before this second result of 8.1 was obtained, a second inoculation was received which produced the same three-week delayed increase (as the first inoculation), showing itself in the third serum test where the value had increased from 8.1 to 8.9 in only one week, representing a gradient increase of 59 degrees in the plot line, and a 20 degree (or 50%) increase in severity above the 1st reaction results. Total WCC values had thus increased about 80% above normal levels over 9.5 weeks.
The electronic graph generated herein for Figure 2(a) does display some visual limitation. The 2nd gradient increase is more clearly evident in the hand drawn (HD) graphs attached to this work , which are drawn to a larger format permitting greater accuracy down to 0.5 mm. The HD graph for Figure 2(a) is shown with the second WCC reading (for the 28th Jan) remaining at the same level of 5.5 as the control date (5th Jan), so that both pre-vaccination scenarios could be presented for this study, ie: where the WCC remained steady at 5.5 (in the HD graph), or, whether it (more probably) had dropped to c.5.0 immediately before inoculation (in the electronic graph). The difference here is academic. More importantly, the protractor readings from the HD graph, show a 1st gradient increase of 36 degrees, and a 2nd gradient increase of 52 degrees, and a difference in severity between both of 16 degrees. The second increase is visually more evident in the HD graph.
Thus in either format (electronic vss hand drawn), the 2nd gradient increase was more severe than the 1st gradient increase by 16 - 20 degrees, and both gradient increases occurred following exposure to the same drug (the vaccine). The 2nd, and greater gradient increase, therefore demonstrates an actual Positive Rechallenge event indicating the body’s stronger response to re-exposure to the same drug – measurable here in graphic presentation, and seen as the sharp increase from 8.1 to 8.9 in only 1 week.
A Positive Rechallenge is a recurrence of the same illness, with it’s symptoms and pathologies, but with a marked increase in severity or intensity, after the patient’s re-exposure to the same drug that caused the first reaction. This phenomenon is literally demonstrated above in Figure 2(a). Dr. Peter Fletcher, Chief Scientific Officer and Senior Principle Medical Officer of the UK’s Committee on Safety of Medicines (CSM), has stated: “The CSM has always accepted that positive rechallenge in the absence of other equivalent and credible causes has to be accepted as a causal relationship.” He further emphasized in the same paragraph, “the great importance of positive rechallenge cases which, for all practical purposes, prove causality.” (Wakefield 2011, i).
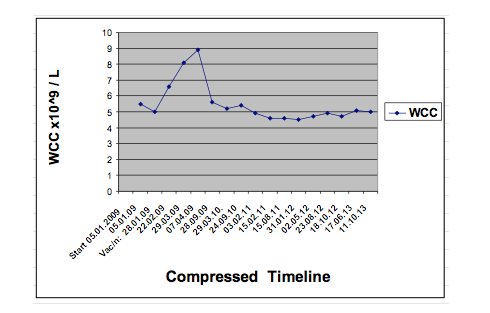
Figure 2 (b) : Chronological progression of White blood Cell Count (WCC) in Paul Taggert following Hepatitis B vaccination.
Figure 2 (b): This second view does not show the Positive Rechallenge (2nd gradient increase) due to the compression of the timescale. The compression has had the effect of rendering each interval along the Y axis to be of equal spacing, thus causing the second gradient increase at the 29.03.09 marker to be stretched longer and lower than what it actually is in real time. What this alternative graph does show, is the return to average pattern for WCC values after the 28.09.09 marker. Total timeline for this data is about 4 years and 8 months.
The values plotted here clearly demonstrate a massive disruption to WBC population following vaccination, requiring some 8 months before total concentrations settled down to routine values. In contrast, the average WCC value between 29.3.10 and 17.06.13 is 4.86 (x10^9/L), demonstrating a significant difference to the acute phase population evident early in the timescale. As this average value would incorporate seasonal viruses and climate changes, the average non-viral WCC value is likely to be about 4.62, as Figure 2(b) and Table 2 above suggests. These average white cell population values show a historical pattern for the author’s genotypic heredity.
WHITE BLOOD CELL SUBSETS:
NEUTROPHILS AND LYMPHOCYTES:
Within the WBC immune family there are two major subsets known as neutrophils and lymphocytes. Table 2 shows the post-vaccination responses of these two subsets. Both subsets are active immune markers for infection, trauma, auto immune disorders, pregnancy, drug side effects, and chemical poisoning amongst others. However, there is no real consensus in the literature as to how each of these subsets react. Reviewer’s findings display a marked variability and were at best limited to broad generalizations. To claim for example, that neutrophil count increases only from bacterial infection, while lymphocytes increase only from viral infection, would require the entire human genome to be uniform - which is obviously not the case. Inoue (2012) correctly noted that in numerous studies neutrophilia alone, had variable sensitivity and specificity as a possible predictor of bacterial infection in young children with fever. Inoue noted that total WBC and specific neutrophil counts alone are not sensitive or specific enough to accurately predict bacterial infection.
What does appear uniform is that either subset can react or inflame from any antagonist or pathogen or contaminant, according to the genetic constitution of the individual. In other words, bacterial infections can cause neutrophilia or neutropenia, or lymphocytosis or lymphopenia; depending on the nature of the pathogen, the phase of illness, and the genotype of the patient. The same can be said of viral infections, trauma, drugs, toxins, etc. Given the diversity of the human genome, it is understandable that subset responses will therefore vary according to the different genetic tools held by each individual, and to the nature of the stimuli. This explains why people’s reactions vary to different infections, drugs, toxins, or traumas. The obvious conclusion is that WCC disruptions have modest discriminatory power in identifying pathogens, and if specific pathogenic tests return negative results, then any disruption to WBC subsets is pointing to other causes. A process of elimination is therefore required, where serology and symptoms are closely compared with a patient’s environmental and clinical history, as is the case for this study.
In the case of this investigation, the author has never displayed such severe and chronic irregularities to enzyme and WCC patterns, in any pathology tests before the vaccinations of early 2009. Furthermore, the possibility of pathogenic infection or pre-existing conditions has already been eliminated via the extensive testing and findings of Tables 2 & 3. The neutrophil and lymphocyte patterns after the inoculation of 28.01.09 not only show massive changes, but also remained unstable for more than 3 years before settling down to routine values. These changes are illustrated in Figure 3 below, and are seen as severe rises and falls in the graph’s plot-lines.
In reviewing the total WCC response to vaccination, it was demonstrated that an upheaval in total values occurred following vaccination (Figs 2 a & b), eventually returning to routine levels. Likewise, a similar but extended pattern of upheaval is visibly demonstrated for the neutrophil and lymphocyte data. The neutrophil count in Table 2 showed an increase from 52% to 75% while the lymphocytes decreased to half their normal levels, ie: from 34% to 16%. The massive increase in neutrophils corresponds to the medical condition known as Neutrophilia, where neutrophil ratios increase to above 70% of the total. Simultaneously, the condition known as Lymphopenia occurred, which is where the lymphocyte ratio fell below 20%.
Figure 2 (b): This second view does not show the Positive Rechallenge (2nd gradient increase) due to the compression of the timescale. The compression has had the effect of rendering each interval along the Y axis to be of equal spacing, thus causing the second gradient increase at the 29.03.09 marker to be stretched longer and lower than what it actually is in real time. What this alternative graph does show, is the return to average pattern for WCC values after the 28.09.09 marker. Total timeline for this data is about 4 years and 8 months.
The values plotted here clearly demonstrate a massive disruption to WBC population following vaccination, requiring some 8 months before total concentrations settled down to routine values. In contrast, the average WCC value between 29.3.10 and 17.06.13 is 4.86 (x10^9/L), demonstrating a significant difference to the acute phase population evident early in the timescale. As this average value would incorporate seasonal viruses and climate changes, the average non-viral WCC value is likely to be about 4.62, as Figure 2(b) and Table 2 above suggests. These average white cell population values show a historical pattern for the author’s genotypic heredity.
WHITE BLOOD CELL SUBSETS:
NEUTROPHILS AND LYMPHOCYTES:
Within the WBC immune family there are two major subsets known as neutrophils and lymphocytes. Table 2 shows the post-vaccination responses of these two subsets. Both subsets are active immune markers for infection, trauma, auto immune disorders, pregnancy, drug side effects, and chemical poisoning amongst others. However, there is no real consensus in the literature as to how each of these subsets react. Reviewer’s findings display a marked variability and were at best limited to broad generalizations. To claim for example, that neutrophil count increases only from bacterial infection, while lymphocytes increase only from viral infection, would require the entire human genome to be uniform - which is obviously not the case. Inoue (2012) correctly noted that in numerous studies neutrophilia alone, had variable sensitivity and specificity as a possible predictor of bacterial infection in young children with fever. Inoue noted that total WBC and specific neutrophil counts alone are not sensitive or specific enough to accurately predict bacterial infection.
What does appear uniform is that either subset can react or inflame from any antagonist or pathogen or contaminant, according to the genetic constitution of the individual. In other words, bacterial infections can cause neutrophilia or neutropenia, or lymphocytosis or lymphopenia; depending on the nature of the pathogen, the phase of illness, and the genotype of the patient. The same can be said of viral infections, trauma, drugs, toxins, etc. Given the diversity of the human genome, it is understandable that subset responses will therefore vary according to the different genetic tools held by each individual, and to the nature of the stimuli. This explains why people’s reactions vary to different infections, drugs, toxins, or traumas. The obvious conclusion is that WCC disruptions have modest discriminatory power in identifying pathogens, and if specific pathogenic tests return negative results, then any disruption to WBC subsets is pointing to other causes. A process of elimination is therefore required, where serology and symptoms are closely compared with a patient’s environmental and clinical history, as is the case for this study.
In the case of this investigation, the author has never displayed such severe and chronic irregularities to enzyme and WCC patterns, in any pathology tests before the vaccinations of early 2009. Furthermore, the possibility of pathogenic infection or pre-existing conditions has already been eliminated via the extensive testing and findings of Tables 2 & 3. The neutrophil and lymphocyte patterns after the inoculation of 28.01.09 not only show massive changes, but also remained unstable for more than 3 years before settling down to routine values. These changes are illustrated in Figure 3 below, and are seen as severe rises and falls in the graph’s plot-lines.
In reviewing the total WCC response to vaccination, it was demonstrated that an upheaval in total values occurred following vaccination (Figs 2 a & b), eventually returning to routine levels. Likewise, a similar but extended pattern of upheaval is visibly demonstrated for the neutrophil and lymphocyte data. The neutrophil count in Table 2 showed an increase from 52% to 75% while the lymphocytes decreased to half their normal levels, ie: from 34% to 16%. The massive increase in neutrophils corresponds to the medical condition known as Neutrophilia, where neutrophil ratios increase to above 70% of the total. Simultaneously, the condition known as Lymphopenia occurred, which is where the lymphocyte ratio fell below 20%.
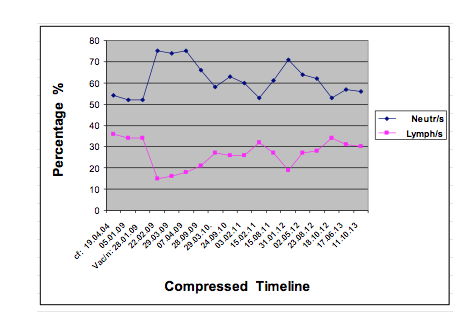
Figure 3: Changes in Neutrophil and Lymphocyte concentrations in Paul Taggert following Hepatitis B vaccination.
The causes of neutrophilia are varied, and include drug and chemical traumas. Normal neutrophil populations have a reference range usually between 50 and 60% of the total WCC. Above 70%, as already stated, is medically significant. Of the 17 FBC’s performed for this investigation (Table 2), 10 tests returned figures of over 60% and four tests were over 70%. The highest count for neutrophils returned a figure of 75% in Table 2, which persisted mostly during the months of the acute phase of injury. In contrast, the pre-vaccination neutrophil population was only 52% of the total WCC.
If the author’s pre-vaccination subsets were added to Figure 3, using two routine neutrophil and lymphocyte test results that were recorded before the injury (one test performed on 19.04.2004 and the other test performed on 05.01.2009) – adding these as an arbitrary repeating pattern (as would be indicative in routine health), such an addition would appear as 2 separate plot lines roughly in parallel and roughly ‘straight’, and very different from the post-vaccination irregular plot lines.
This arbitrary addition is illustrated in Figure 4 below and is identified in the side key as ‘Routine Nt’s and Routine Ly’s’. The comparative data for these pre-vaccination subsets is listed in Appendix 1 (table for Figures 3 and 4).
The causes of neutrophilia are varied, and include drug and chemical traumas. Normal neutrophil populations have a reference range usually between 50 and 60% of the total WCC. Above 70%, as already stated, is medically significant. Of the 17 FBC’s performed for this investigation (Table 2), 10 tests returned figures of over 60% and four tests were over 70%. The highest count for neutrophils returned a figure of 75% in Table 2, which persisted mostly during the months of the acute phase of injury. In contrast, the pre-vaccination neutrophil population was only 52% of the total WCC.
If the author’s pre-vaccination subsets were added to Figure 3, using two routine neutrophil and lymphocyte test results that were recorded before the injury (one test performed on 19.04.2004 and the other test performed on 05.01.2009) – adding these as an arbitrary repeating pattern (as would be indicative in routine health), such an addition would appear as 2 separate plot lines roughly in parallel and roughly ‘straight’, and very different from the post-vaccination irregular plot lines.
This arbitrary addition is illustrated in Figure 4 below and is identified in the side key as ‘Routine Nt’s and Routine Ly’s’. The comparative data for these pre-vaccination subsets is listed in Appendix 1 (table for Figures 3 and 4).
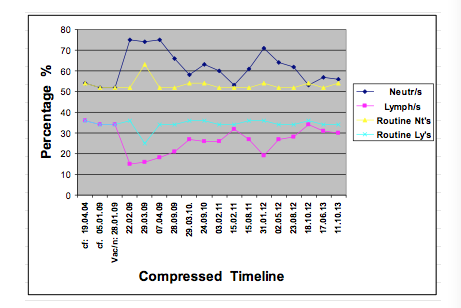
Figure 4: Pre-vaccination (routine) and Post-vaccination WCC subsets combined.
For added comparison, the serology results of a transient flu virus which hit hard on Australia’s population in the winter of 2007, which the author also contracted, have been included in these Routine plot lines. This short seasonal virus is inserted at the 5th marker in the graph’s timeline, ie: at the 29.03.09 marker, for easy comparison. Note – the most response this nasty virus could incite from the author’s white cell subsets, was a much smaller spike of 63% neutrophils and 25% lymphocytes (but only 4.6 WCC), compared to the massive and eruptive spike generated by the post-vaccination destabilisation in Figs. 2 & 3. After this seasonal flu had passed, the author returned to work with no latent symptoms whatsoever, and maintained normal workloads thereafter. This arbitrary comparison however, has the advantage of clearly demonstrating just how robust the author’s immune system was before 2009, by the nil to moderate changes in WCC subsets during the cycles of routine health.
In conclusion, as no pathogenic infections or pre-existing conditions could be identified from Table 3 data, the relationship between the neutrophilia and the vaccine drug is therefore strongly supported, and expressed in part as an acute inflammatory response of the total and differential immune cells. In the absence of other identifiable causes, these significant, sudden and erratic shifts point to a drug induced pathogenesis brought about by the HBV inoculations.
LYMPHOCYTE SUBSETS: AUTOIMMUNE DYSREGULATION:
SUB-SECTIONS:
i): Definitions
ii): Author’s persisting autoimmune cytotoxicity (Table 5)
iii): Author’s CFS correlation (Table 6)
iv): Author’s MS correlation (Table 7)
v): Warnings of Hepatitis B Vaccine (HBV) Toxicity.
i): Definitions:
Genotype: Is the inherited genetic characteristics an organism carries within its DNA. That is, the genetic code of an individual. The human genome has a complement of 46 chromosomes per gene. There are many variants (genotypes) within this genome.
Phenotype: Is the outward showing of physical appearance or chemical behavior of an organism or cell type. The genetic expression of such outward traits, has been altered as a result of its interaction with its environment. The genetic modifications are a change of expression, not a change of genetic complement.
Thus: genotype + environmental pressures + random variation = phenotype.
Cytokines: Are small mediatory proteins secreted by a broad range of cells such as B Cells, NK cells, T Cells, dendritic cells, eosinophils, macrophages, mast cells, and neutrophils. Cytokines are also referred to as polypeptide cell regulators, and as immunomodulating agents. They are vital in triggering varying forms of immune defenses. Cytokine’s specialised abilities affect cell signaling, cell growth, cell expression, cell activation or inhibition, and modulation of cell populations.
Cytokines are many in number and act through receptors, and may be divided into Pro-inflammatory and Anti-inflammatory types, because they can incite or reduce tissue inflammation. They have also been arbitrarily divided into several subfamilies – these being: Chemokines, Colony stimulating factors, Interferons, Interleukins, Lymphokines, and Monokines. Liles and Van Voorhis (1992, 1573-80) have reviewed 42 mammalian cytokines, providing a ready reference guide to these important molecular mechanisms.
Cytokines are susceptible to dysregulation leading to autoimmune imbalances and disease states. Interferons and interleukins are used as drugs to remedy or decrease some of these disorders. When genetic damage occurs, cytokine communication and control can become disrupted resulting in out-of-control cytotoxicity states, including inflammatory conditions called cytokine storms. Several models have been developed to describe differing cytokine patterns in various diseases and disorders (see below). Not all cytokines fit neatly into each model due to their cross-regulatory properties and complex interaction.
Cytolytic: Is where an organism, substance, or cell possesses a solvent or destructive action upon other cells. Some forms of cytolysis can induce autoimmune disorder.
Cytotoxicity: (cell – toxic). Is the degree to which an organism, process, agent, substance, or molecule; is hazardous to the function and survival of other living cells.
Eg: Heavy metals (mercury, aluminium) are known neurotoxins and carcinogens.
Lymphocyte-mediated Cytotoxicity: Is the unwanted destruction of host cells by various types of lymphocytes. The cytolytic process may be detrimental to the host’s overall health, resulting in various autoimmune states. Sources of lymphocyte-
mediated cytotoxicity include:
1): T Cells which switch from restricted to non-restricted, & become indiscriminate.
2): Over-production or over-activation of naturally occurring NK cells.
Non-MHC-Restricted T Cells: (or non-MHCR T cells):
Refers to specific lymphocytes that do not have safety restriction towards Major Histocompatibility (MHC) peptides (antigens). Their interaction and potential cytotoxicity is NK-like in severity, resulting in unrestricted aggression not only towards foreign peptides, but also towards certain host peptides. The increase in these cells is induced by an uncontrolled secretion of cytokine production, itself a shift brought about by the immunogenic activity of some vaccines. Thus, self-tolerating autoimmunity becomes disrupted due to an increase in non-MHCR T cell activity.
T Cells and T Helper Nomenclature:
T Cell lymphocytes represent a major component of the Adaptive immunity and include the following phenotypes (with their relative CD surface proteins):
T Suppressor cells (CD8), T Cytotoxic Cells (CD56), and T Helper cells (CD4).
Mature T Helper cells (Th) have several roles: some act as effectors by secreting cytokines, some retain antigenic memory for later action, and some are self-limiting regulators. Three popular models have been formulated to describe the alternate forms of Th immune defense. These models focus upon the common regulation of humoral and T cell-mediated host responses to antigens.
These models are: A) HpS Model. B) Th Model. C) Th-like Model.
A): Hypersensitivity Model (or HpS Model):
Developed in 1963 by Coombs and Gell (p.317-37) this simple model attempts to categorise T Helper activation of cytokines to ultra low level antigen exposure. There are four types of immune responses proposed under this model. These are:
Type 1 HpS:
This is the most common type of sensitivity reaction and involves the generation of IgE antibodies towards antigens which the host is genetically sensitive to. Autoantigenic over-activation of T1-HpS gives rise to rapid response injuries (allergies) such as anaphylaxis (eg: from nuts or stings), asthma, hay fever, coeliac, eczema, hives and rashes.
Type 2 HpS:
This type of sensitivity involves the generation of low affinity or auto-specific antibodies. T cell effectors similar to the Th 2 cytokines are also thought to be involved. Autoantigenic over-activation of T 2-HpS can lead to Grave’s disease.
Type 3 HpS:
This type of sensitivity also involves the generation of low affinity or auto-specific antibodies. The same T cells as in the Th2 cytokines are thought to be involved. Autoantigenic over-activation of T3-HpS can lead to delayed response injuries (DRI’s) such as lupus (SLE), and Rheumatoid conditions.
Type 4 HpS:
This type of sensitivity generates non-antibody delayed injury states, directly as a result of over-stimulation of the immunity, particularly of lymphocytes and macrophages, leading to pro-inflammatory cytokine releases. Autoantigenic over-activation of T4-HpS can result from poor diet, drugs, and toxins; and can lead to DRI’s such as Type 1 diabetes and various neurological states.
B): T Helper Model (or Th Model):
Developed in 1971 by Parish (p.21-47) the Th model began as a simple division of immune responses into two groups (Type 1 and Type 2) depending on the proportional relationship of Humoral (antibody) lymphocytes versus Cellular (T and NK) lymphocytes. The Type hypothesis was further developed by Mosmann et. al. (1986, 2348-57) into the Th1 / Th2 model which categorises cytokines as to their production and cellular origins. Lucy et.al. (1996, 532-62) and Spellberg and Edwards (2001, 76-102) are amongst other researchers who have further reviewed the model. Type 1 / Type 2 and Th1 / Th2 are now used interchangeably. Th cells are driven by cytokine patterns, which cross-regulate each other in their activation / suppression roles, so that when one Type increases the other decreases. The profiling of these patterns within this model, serves to identify imbalances and dysregulation where these arise in various diseases and autoimmune states. These patterns are:
T Helper Cell - Type 1 cytokine pattern (Th 1):
The natural occurrence of this pattern is as a Cellular immune response, mainly in partnership with macrophages. IgG – B cells and other T cells (CD4 and CD8) can be secondary effectors. A typical Th1 response is tissue pain, redness, swelling and heat after intracellular infections occur from bacteria and protozoa. Autoantigenic over-activation of Th1 from poor diet, drugs, and toxins; can lead to delayed response injuries (DRI) such as Type 1 diabetes and various neurological states.
Sub-type Th17: This pattern arises in partnership with neutrophils. IgM and IgA – B cells can be secondary effectors. A Th17 response occurs from extracellular infection from bacteria and fungi. Autoantigenic over-activation of Th17 can lead to DRI’s such as Rheumatoid conditions.
T Helper Cell - Type 2 cytokine pattern (Th 2):
The natural occurrence of this pattern is as a Humoral immune response, resulting in high titers of antibody production of IgE – B cells. Infections from multicellular parasites such as worms (Helminths) can promote Th2 responses. Autoantigenic over-activation of Th2 gives rise to rapid response injuries (allergies), such as asthma, hayfever, lupus, nuts, stings and rashes, eosinophilia, basophilia, pulmonary CFA, and extensive mast cell degranulation.
T Helper Cell – Type aB cytokine pattern (ThaB):
This pattern occurs as a combination immune response, where both Innate and Adaptive immune faculties are involved. The main partnership is between NK and T cells, although IgG – B cells can also act as secondary effectors. ThaB responses arise when infections occur from viruses. Autoantigenic over-activation of ThaB can lead to Grave’s disease, Chronic Fatigue and various neurological states.
C): Th-like (Type 1 / Type 2) Model:
This is a variation of the Th model. This model first suggested by Bloom et.al. in 1992, closely follows the Th model above, where Type1 means Th1-like, and Type 2 means Th2-like. However, this model includes both T and non-T Cell cytokines in its nomenclature, and emphasizes the functional response of cytokines rather than their cellular origins. Type 1 represents a strong cellular response with normal to increased production of various interleukin and other cytokines. Type 2 represents an impaired cellular response with increased B Cell activities.
ii): Author’s Persisting Autoimmune Cytotoxicity:
In recalling the common practice of inducing cytotoxicity discussed in the Prologue of this report, and how researchers are able to transform passive lymphocytes into aggressive killer phenotypes; we now progress to examine a very similar cytotoxic process evident in the author’s serology.
Remembering the earlier Chimpanzee comparison, where a 2% genetic variation produces an animal of many differences to humans, likewise a small vaccine-mediated alteration within a genetically susceptible person can induce many differences to that individual’s system protocols. The result being out-of-control cytotoxicity and subsequent autoimmune shift. The thousands of personal injury claims registered worldwide testify of the cytotoxic potential of certain vaccines.
In the author’s serology findings, the data clearly shows significant changes to WCC and subset arrangements after a lapse of a few weeks, following the receipt of HBV injections. The devastating Positive Rechallenge assault to immune ranks that followed, subsequently led to a 3.5 year hiatus in routine function before the regiment of WBC’s could settle and reorganize. The delayed timing and duration of the acute phase of the author’s injury demonstrates a normal protective immune response. The first reaction to the vaccine was delayed followed by a Positive Rechallenge delay to the second injection. The primary cells used to mount the acute reaction were neutrophils (Figs 3 & 4). This innate-driven protective pattern is typical of a Th 17 profile in the Th Model, or a Type 4 response in the HpS Model.
However, subsequent serology tests demonstrated that B cells did not appear to be primary effectors during any of the injury phases, as no B-driven antibodies could be identified from the pathogenic tests, and no autotoxic B elevations could be identified in the Lymphocyte Surface Marker tests. Since B autoreactivity is involved in Th 1 responses, yet this did not show, the author’s immune profile must contain another aspect of dualistic origin.
After the neutrophil (acute) phase had subsided, an alternative profile manifested in the form of allergic type food intolerances to breads, during the intermediate phase of injury and after. The author found that wheaten foods could no longer be tolerated – which gave rise to sudden and long exhaustion bouts; and antibiotics and certain herb teas caused rapid cardio-metabolic distress; while some stored and processed foods caused rapid ‘food poisoning –like’ reactions, which were otherwise well tolerated by other family members. These clinical manifestations demonstrated an immune shift toward a new hypersensitive profile synonymous with a Th 2 pattern. However, B cell autoreactivity was missing as noted above, and eosinphilia and basophilia elevations were also absent in the serology. Thus, the Th 2 profile was also incomplete.
Since components of both Th 1 and Th 2 patterns are evident in the author’s immune response, and a chronic immune profile has developed showing a combination of elements; the final profile could arbitrarily be described as a Th- aB pattern. This combination pattern is supported in the serology, signified by a sustained cell-mediated release of elevated levels of neutrophils; followed by releases of Natural Killer (NK) cells and NK Receptors, in partnership with non-MHC-Restricted T cells. Both NK and non-MHC-R T cells are known to be particularly promiscuous phenotypes toward neighbouring cells and tissues. The sustained cellular elevations are demonstrated in Table 5 below. The partnership between Innate NK cells and Adaptive T cells fits the aB pattern, and is further indicated by the viral component of the offending vaccine, given that aB patterns are triggered by viral antigens. Since NK and T cells are both lymphocytes, their release also suggests adjuvant-mediated stimulation which once initiated, has failed to switch off. The aB pattern arbitrarily corresponds to Type 2 in the HpS model.
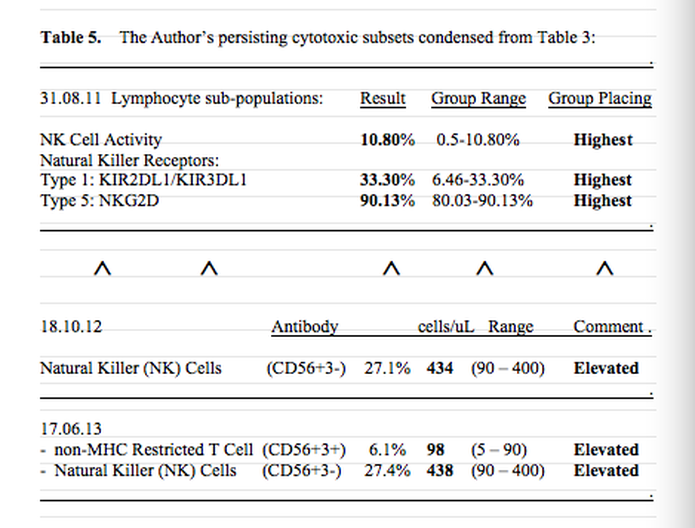
Table 5 clearly shows that non-MHC-R T cells and NK cells expressed as CD56 phenotypes are elevated above the normal reference range in the last two tests, and when compared to other sufferers in the severe group tested on 31.8.11, the author’s range in that group took highest placing. Thus, while the numerical increases in this table appear only to be marginal, the elevated levels are sufficient to cause significant illness in the author, particularly when reconciling the author’s data placing in the group of seven severe sufferers. These elevated levels strongly implicate a change in genetic regulation towards CD56 expression, representing an unnatural and potently stimulated immune activation following vaccination, which has failed to switch off.
After the passing of 5 years, the elevated ranks of lymphocytes appear to be chronically resident, strongly evoking a vaccine-mediated autotoxic immune shift which is potentially irreversible with current technology. Excessive CD56 phenotypes induced within a balanced operating physiology can have only one outcome – internal trouble and destabilisation. Such autoimmune dysregulation leads to a domino effect upon other operating body systems, as is evidenced in the author’s constellation of symptoms listed in Tables 7 & 8 following, and the durational phases those symptoms are expressed within. Thus, the law of genetic sensitivity discussed earlier in the Prologue, appears reflected in the system changes to the author’s health.
CD56 auto aggression was investigated by Antel et. al. (1998) who found that high CD56 activated T cell lines were able to induce significant lysis of human oligodendrocytes (OL), which are the progenitor cells for myelin tissue. Myeloid destruction is the process that forms Multiple Sclerosis (MS) states. The same cell lines were found not to be cytotoxic under resting conditions (ie: as routine passive phenotypes). Quoting from their discussion, Antel et.al. noted:
“Our current results indicate that MBP-reactive CD4 T-cells can acquire the capacity to induce non-MHC-restricted cytotoxicity. Notably, OL-directed cytotoxicity was associated with expression of CD56 on the T-cells. We further found that our 251 glioma cell line….. was susceptible to lysis by CD56-expressing MBP- reactive T cell lines. Recently stimulated cells were highly activated, phenotypically showed increased CD56, and functionally were also cytotoxic than the same cells under resting conditions…. Our results….further indicate the crucial role of cell-surface molecules involved in effector-target cell interactions in determining whether… injury will occur. These results indicate that these cells do have the intrinsic capacity to induce injury….” Antel et. al. also suggested that the lysis of some cells involved the fragmentation of DNA within cell nuclei via both perforin (a toxic protein) and fas-dependent pathways.
Faure (2005) provided similar evidence of cytotoxicity by describing a breakdown in immune recognition processes where the viral genome of HBV’s not only resembles human protein in general, but closely resembles myelin basic protein (which covers our nerve axons). This similarity (or mimicking) of the vaccine’s denatured protein to our own myelin protein, leads to a process of failure in recognition between the two proteins, triggering a cascade of cytotoxic expression because the vaccinated immune system cannot discern between the two. The newly altered expression equates to a combative state of confusion, resulting in the destruction of myeloid sheathing (a MS state), by previously friendly immune cells.
Other phenotypic activation, additional to CD56 phenotyping, appears also to arise from immune stimulation. von Geldern et.al. (2006, 2347-58) investigated the mechanisms of phenotypic activation and found that such activation occurred when protein cell regulators were artificially manipulated. Their experiments confirmed that short term stimulation induces non-MHC-restricted T cell activation and sustained cytokine and chemokine secretion, involving CD4+ and CD8+ phenotypes. They noted the following:
Pg 2350): “….various cytokine-based activation protocols have been shown to induce ‘antigen-independent’ T cell responses. Cytokine stimulation of peripheral lymphocytes results in ‘non-specific’ T cell responses detected as non-MHC-restricted cytotoxicity 1_6. TCR-dependant activation…. as well as TCR-independent stimulation….revealed the potential of peripheral T cells to behave as NK cells by switching to a non-MHC-restricted cytotoxicity pattern 6_9…..Common features of non-MHC-restricted T cells include their polyclonal activation via cytokine receptor triggering, the production of various cytokines and their non-MHC-restricted cytotoxicity. Recent evidence suggests the presence of NK-like cells in vivo in the gut of celiac patients….These CTL attacked autologous intestinal epithelial cells in a non-MHC-restricted fashion 13_14.”
von Geldern et. al. go on to describe their methodology and show how CD4+ and CD8+ cells can be ‘turned’ from passive to toxic without CD56 phenotyping, stating:
“CD56 was not found on CD4+ or CD8+ T cells” (pg 2354),
but that cytokine stimulation can induce a pattern of T cell phenotyping which is independent of antigen exposure, and that:
“non-MHC-restricted cytolytic pattern is strikingly similar to NK cell activity”.
Transmuting these results into the parameters exhibited in Table 5, we find the pattern of stimulation >> dysregulation to be confirmed. A vaccine was injected twice. Two severe reactions followed after each inoculation, the second leading to serious injury. The adjuvant or viral component (or both), shocked the liver into an apoptotic cascade, while also inducing the secretion of excessive amounts of cytokines. Massive releases of liver enzymes ensued, accompanied by large increases in WBC’s. After the ‘dust’ settled, the production of activated receptors (AR) failed to switch off due to the lingering effects of adjuvation or mimicry (or both), while sufficient numbers of inhibitory receptors (IR) which function to counter such increases, could not respond. Thus, after the initial shock, the immune system fell into a condition where it could no longer abrogate aggressive phenotypes that exceed system protocols. The persisting elevated NK and unrestricted T cell phenotypes in Table 5 mirror that breakdown in immune regulation. This entire process is a picture of dysregulation, where the immune system still functions but some of its protocols remain impaired.
What the experimental stimulation employed by immunotherapists shows is that:
Ø Researchers admit to inducing cytotoxic changes in undisturbed immune cells.
Ø Immune responses can occur outside of antigen-dependant safety protocols.
Ø Activated cytokine protocols can lead to unfavourable NK and T cell responses.
Ø Such activation can lead to toxic concentrations of aggressive phenotypes.
Ø CD56 phenotypes are not the only type of autoimmune cytotoxicity states.
Ø Normal MHC-restricted T cells can be transformed into NK-like T cells, ie: restricted T cells are ‘turned’ into non-restricted’ cells, with free aggression.
Ø Experiments are designed with the goal of inducing potent therapeutic remedies.
Ø “occasional high but variable and unpredictable clinical responses 39_42” do occur (von Geldern et.al. 2006, 2359).
Ø Researchers are aware that manipulation of the immune system can produce unpredictable and out-of-control autoimmune cytotoxicity.
What all this confirms is that the immune system is not some ethereal system that has a lifetime warranty and remains impervious to change, as vaccine campaigners hope. The truth is exactly the opposite. The immune system is easily shifted with often detrimental results, leading to damage that is often irreversible. The mass corruption of immune systems that we have seen in modern times can only be attributed to the mass deployment of immune stimulation devices – vaccines. This injurious process is not a new revelation by any means – researchers have known of the susceptibility of the immune system to manipulation for decades.
Thus, modern gene expression studies are revealing a picture of immune function impairment involving artificially shifted immune responses, cytolytic changes to beneficial protector cells, breakdowns in friendly recognition procedures, lysidic invasion of CD56 and other aggressive phenotypes, and resultant chronic injury states inflicted on unsuspecting recipients. In short, certain immune defenses that were once protective of their hosts, are converted by vaccine interference into hostile factions, which then not only combat traditional pathogens but also turn on their own hosts because they cannot switch off. The link between the author’s excessive compliment of cytotoxic phenotypes and the findings of the above researchers, strongly suggests a causal relationship between phenotypic activation and the author’s symptoms of injury. This cytotoxic link may be framed as follows:
· Total numbers of CD56 cytotoxic phenotypes are elevated, as Table 5 shows.
· NK cell activity for the author was highest in the group of seven test subjects.
· No pathogens or pre-existing conditions could be identified from the serology.
· No pathogenic justification exists therefore, for an increase in CD56 ranks.
· The action of vaccine stimulation is the only event in the author’s clinical history that could have induced such phenotypic conversion.
· The increased CD56’s must have target zones, otherwise why have such numbers?
· The target orientation of the immune defenses may now have changed.
· The author’s symptom states strongly identifies the new source of targeting.
· 15 body systems were disrupted soon after vaccination, with 12 remaining chronic.
· Marginal increases in the test group’s CD56 expression, appear to be sufficient to cause major disruption to health.
· Abnormal differentiation in other B cell, T cell, and NK cell lines might also contribute to injury states, such as CD 16 and CD 4 cytotoxic phenotypes.
· Out-of-control genetic self-targeting constitutes classic autoimmune injury.
These unnatural program changes therefore represent a dysregulation of inherited operational arrangements and may include any of the following mechanisms and outcomes:
Þ DNA base modifications, strand fragmentations, or portional recodes.
Þ Changes to existing histocompatibility arrangements.
Þ Changes to cell transport pathways, including faulty signaling.
Þ Alterations in protein specificities within or between cell lineages (eg: myeloid cells), due to the introduction of foreign peptides or modified proteins.
Þ Changes in friendly recognition resulting in death by mimickry.
Þ Shifts in cytokine and receptor balances causing excesses or deficiencies.
Þ Unnaturally high concentrations of aggressive cell phenotypes.
Þ Lysis of beneficial bacteria and/or mucosal barriers in the GIT.
Þ Lysis of mitochondria resulting in mass cell death (ie: apoptotic cascade).
Þ Impaired Krebs Cycle / impaired Methylation Cycle.
All of these injurious processes lead to chronic injury states such as Chronic Fatigue, Multiple Sclerosis, Irritable Bowel, and many other neurological and metabolic states.
iii): Author’s CFS Correlation:
The author was invited to participate in a Chronic Fatigue Syndrome (CFS) university case control study, which included serology investigations into the WBC immune subpopulations of a small group of CFS sufferer’s. Seven members of this group of about 200 people were regarded by the faculty staff as being severely impaired, including the author. The immune cell subpopulations under investigation included lymphocyte surface marker examination. The testing was undertaken to determine how sufferers of chronic fatigue differed immunologically from individuals of normal health. After the case study concluded, the author continued testing for irregularities within lymphocyte lineages including B cell, T cell, and NK cell sub-populations. The findings of these autoimmune markers are shown in Table 3, and have been discussed in greater detail in the previous subdivision relating to Table 5.
When Gherardi (2003) investigated autoimmune states as possible manifestations of vaccination sensitization in France, Gherardi described artificially shifted immune responses forming chronic fatigue syndromes, caused by aluminium adjuvants in certain vaccines. Other gene expression studies have also described shifted immunogenic responses giving credence to the growing body of evidence that vaccine damage is correctly a pathogenetic concept. Similar to Gherardi’s revelations, Nancy and Shoenfeld (2008) also implicated the onset of CFS in a patient in their study. They stated: “CFS etiology is multi-factorial commonly triggered by infectious agents. Vaccines, induce an immune response similarly to infections, and may trigger just like infections autoimmune diseases, CFS and fibromyalgia. Furthermore vaccines contain an adjuvant which enhances their immune stimulation …..Our patient illness started following hepatitis-B vaccine, suggesting that it was caused or accelerated by vaccination.”
The pathological immune stimulation Gherardi and other researchers have alerted to, involves alterations to the behavior of some lymphocyte lines rendering them with new aggressive expression towards their siblings and neighbours. As previously described, lineages in the Adaptive immune system evolve under chemo-genetic intervention into new activated phenotypes that infiltrate tissues, organs and pathways causing damage – an auto-immune coup` in other words. The resulting damage from such intervention is the development of neurological and inflammatory disease states such as CFS, GBS, MMF, MND, MS, and SLE; etc.
CFS has been the subject of many studies, including the university study noted above which the author participated in. CFS is clinically characterized by persistent and debilitating fatigue (ie: weakness and loss of stamina), which is not remedied by adequate rest, nutrition and sleep. The condition impairs daily activity and diminishes quality of life indefinitely in victims. Other CFS symptoms include headaches, dizziness, GIT disturbances, muscle pain, joint pain without the swelling, exercise penalty malaise, tender lymph nodes, and cognitive dysfunction such as impaired concentration, memory, mood and sleep.
The laboratory characterisation for CFS has remained elusive because repeatable biochemical markers have been unattainable or inconsistent, leaving diagnosis dependent primarily upon persisting clinical symptoms specific to each individual. In the body of literature investigating the causes of CFS, there are a variety of markers that although not consistent in all cases, do point to causal mechanisms. A list of these potential markers is compiled in Table 6 where comparison is made to the author’s empirical and clinical history. The lack of infectious triggers noted in Table 6 for the author’s CFS, has already been discussed in earlier sections.
As the author’s injury includes the primary symptoms of CFS, it would be logical to expect that some of these markers might be relevant to the author’s case. However, while some of these markers are still in the hypothetical stage, and other markers have not yet been tested in the author’s investigations, presently only three markers exhibit a point of contact with the author’s case history, those being:
- CFS preceded by vaccination (ie: vaccination caused CFS onset)
- Decreased serum Coenzyme Q10 (the energy molecule)
- Mitochondrial degeneration (associated with post-vaccination Liver Toxemia).
Thus, the etiology of synthetically induced CFS via a vaccine mechanism, is significantly more plausible than an infectious etiology, and supported by the positive correlation with the literature markers for post-vaccination onset and chronic liver toxemia.
Table 6 ……………………………………………………………………. > /
Table 6: Potential markers for CFS activation compared to the Author’s case.
.
Potential Markers l Author’s Medical Case
l .
CAUSAL MARKERS:
CFS onset preceded by new virus Last virus 18 months before injury
CFS onset by reactivated old virus No reactivation in serology or period.
CFS preceded by bacterial infection No bacterial infection in serology
CFS preceded by vaccination Yes – following HBV inoculation
BIOLOGICAL MARKERS:
Increased serum CRP CRP constantly normal
Decreased serum NK cells NK cells chronically elevated
Activation of CD 26, 38, 69 T cells None noted –only CD 56 elevated
Elevated serum auto-antibodies ANA, AAM, ANC, DNAA normal
Elevated B Cell phenotypes CD19 B Cells normal
Elevated pro-inflammatory cytokines Cytokine tests ordered >>
Decreased anti-inflammatory cytokines >> Results not supplied
Degranulation of T and NK Cells Untested
Excessive gut hydrogen sulfide (H2S) Untested
Elevated aerobic bacteria in GIT Untested
Elevated LPS for g.n. enterobacteria Untested
Depletion of antioxidants (L-glut./ 8-OHdG) Untested
Elevated serum lactic acid Untested
Decreased serum CoQ10 Yes – significant decrease
Activation of Mast Cells Untested
Mitochondrial degeneration Yes – in Liver Toxemia
Neural Inflammation CSF – IgG negative
iv): Author’s MS Correlation:
The chronic inability to maintain standing or walking for regular durations, together with the diffuse myalgias/dizziness/fatigue/GIT syndrome that the author has endured following HBV inoculations, strongly resembles MS-like autoimmune cytotoxicity even though limited specific serology for MS could not provide positive results. Parallel MS-like states however, without supporting MS pathology are known clinical manifestations for a variety of vaccines, and many vaccine injury reports similarly testify of ‘leg weakness’ and other neurological disorders. Numerous hospital corridors and waiting rooms have been influxed by vaccinated people who have found themselves in sudden and unexpected need of leg braces and wheelie walkers.
Hernan et.al. (2004) noted in their independent UK case control study:
“The OR (odds ratio) of MS for vaccination within 3 years before the index date compared to no vaccination was 3:1…..These findings are consistent with the hypothesis that immunization with the recombinant hepatitis B vaccine is associated with an increased risk of MS….” Mikaeloff et. al. 2009 also noted in their case control study of vaccinated French victims suffering similar neural demyelination between 1994-98; that “the Engerix B vaccine appears to increase this risk, particularly for confirmed multiple sclerosis, in the longer term.”
Girard (2005), who was privy to suppressed surveillance data arising from his consultancy background, stated: “In 25 years of professional life devoted to the study of drug hazards, I have rarely seen an issue clearer than that related to the potential of hepatitis B vaccine to induce auto-immune diseases.” Girard (2007) illustrated the link between the increase of MS states in France after 1994, and the deployment of HBV inoculations. Referring to the French vaccination campaign, he stated:
“Another observation of indisputable significance in post-marketing surveillance was a sharp increase in a disease (MS) whose spontaneous occurrence was miniscule before the introduction of the suspected vaccine…..this dramatic 25-fold increase during a period where mass vaccination against hepatitis B was the most drastic change in the health environment gives enormous credibility to the hypothesis of neurotoxicity linked to this vaccine…..this means that a number of doctors…..had never, in their professional lives, met a patient with MS. Nowadays however, at all social or professional levels, anybody – health professional or not knows of several cases of MS in people around him/her.”
MS and MS-like injuries are devastating conditions to acquire, and usually produce a constellation of symptoms. Authier et. al. (2001, 975) stated:
“The association between MMF and multiple sclerosis-like disorders may give new insights into the controversial issues surrounding vaccinations and demyelinating CNS disorders”.
A compilation of the more common MS symptoms has been listed below in Table 7. The 36 symptoms are commonly found on the major MS websites, and these are correlated to the author’s injury in terms of their phase occurrences and repetition.
iv): Author’s MS Correlation:
The chronic inability to maintain standing or walking for regular durations, together with the diffuse myalgias/dizziness/fatigue/GIT syndrome that the author has endured following HBV inoculations, strongly resembles MS-like autoimmune cytotoxicity even though limited specific serology for MS could not provide positive results. Parallel MS-like states however, without supporting MS pathology are known clinical manifestations for a variety of vaccines, and many vaccine injury reports similarly testify of ‘leg weakness’ and other neurological disorders. Numerous hospital corridors and waiting rooms have been influxed by vaccinated people who have found themselves in sudden and unexpected need of leg braces and wheelie walkers.
Hernan et.al. (2004) noted in their independent UK case control study:
“The OR (odds ratio) of MS for vaccination within 3 years before the index date compared to no vaccination was 3:1…..These findings are consistent with the hypothesis that immunization with the recombinant hepatitis B vaccine is associated with an increased risk of MS….” Mikaeloff et. al. 2009 also noted in their case control study of vaccinated French victims suffering similar neural demyelination between 1994-98; that “the Engerix B vaccine appears to increase this risk, particularly for confirmed multiple sclerosis, in the longer term.”
Girard (2005), who was privy to suppressed surveillance data arising from his consultancy background, stated: “In 25 years of professional life devoted to the study of drug hazards, I have rarely seen an issue clearer than that related to the potential of hepatitis B vaccine to induce auto-immune diseases.” Girard (2007) illustrated the link between the increase of MS states in France after 1994, and the deployment of HBV inoculations. Referring to the French vaccination campaign, he stated:
“Another observation of indisputable significance in post-marketing surveillance was a sharp increase in a disease (MS) whose spontaneous occurrence was miniscule before the introduction of the suspected vaccine…..this dramatic 25-fold increase during a period where mass vaccination against hepatitis B was the most drastic change in the health environment gives enormous credibility to the hypothesis of neurotoxicity linked to this vaccine…..this means that a number of doctors…..had never, in their professional lives, met a patient with MS. Nowadays however, at all social or professional levels, anybody – health professional or not knows of several cases of MS in people around him/her.”
MS and MS-like injuries are devastating conditions to acquire, and usually produce a constellation of symptoms. Authier et. al. (2001, 975) stated:
“The association between MMF and multiple sclerosis-like disorders may give new insights into the controversial issues surrounding vaccinations and demyelinating CNS disorders”.
A compilation of the more common MS symptoms has been listed below in Table 7. The 36 symptoms are commonly found on the major MS websites, and these are correlated to the author’s injury in terms of their phase occurrences and repetition.
After the passing of 5 years, the elevated ranks of lymphocytes appear to be chronically resident, strongly evoking a vaccine-mediated autotoxic immune shift which is potentially irreversible with current technology. Excessive CD56 phenotypes induced within a balanced operating physiology can have only one outcome – internal trouble and destabilisation. Such autoimmune dysregulation leads to a domino effect upon other operating body systems, as is evidenced in the author’s constellation of symptoms listed in Tables 7 & 8 following, and the durational phases those symptoms are expressed within. Thus, the law of genetic sensitivity discussed earlier in the Prologue, appears reflected in the system changes to the author’s health.
CD56 auto aggression was investigated by Antel et. al. (1998) who found that high CD56 activated T cell lines were able to induce significant lysis of human oligodendrocytes (OL), which are the progenitor cells for myelin tissue. Myeloid destruction is the process that forms Multiple Sclerosis (MS) states. The same cell lines were found not to be cytotoxic under resting conditions (ie: as routine passive phenotypes). Quoting from their discussion, Antel et.al. noted:
“Our current results indicate that MBP-reactive CD4 T-cells can acquire the capacity to induce non-MHC-restricted cytotoxicity. Notably, OL-directed cytotoxicity was associated with expression of CD56 on the T-cells. We further found that our 251 glioma cell line….. was susceptible to lysis by CD56-expressing MBP- reactive T cell lines. Recently stimulated cells were highly activated, phenotypically showed increased CD56, and functionally were also cytotoxic than the same cells under resting conditions…. Our results….further indicate the crucial role of cell-surface molecules involved in effector-target cell interactions in determining whether… injury will occur. These results indicate that these cells do have the intrinsic capacity to induce injury….” Antel et. al. also suggested that the lysis of some cells involved the fragmentation of DNA within cell nuclei via both perforin (a toxic protein) and fas-dependent pathways.
Faure (2005) provided similar evidence of cytotoxicity by describing a breakdown in immune recognition processes where the viral genome of HBV’s not only resembles human protein in general, but closely resembles myelin basic protein (which covers our nerve axons). This similarity (or mimicking) of the vaccine’s denatured protein to our own myelin protein, leads to a process of failure in recognition between the two proteins, triggering a cascade of cytotoxic expression because the vaccinated immune system cannot discern between the two. The newly altered expression equates to a combative state of confusion, resulting in the destruction of myeloid sheathing (a MS state), by previously friendly immune cells.
Other phenotypic activation, additional to CD56 phenotyping, appears also to arise from immune stimulation. von Geldern et.al. (2006, 2347-58) investigated the mechanisms of phenotypic activation and found that such activation occurred when protein cell regulators were artificially manipulated. Their experiments confirmed that short term stimulation induces non-MHC-restricted T cell activation and sustained cytokine and chemokine secretion, involving CD4+ and CD8+ phenotypes. They noted the following:
Pg 2350): “….various cytokine-based activation protocols have been shown to induce ‘antigen-independent’ T cell responses. Cytokine stimulation of peripheral lymphocytes results in ‘non-specific’ T cell responses detected as non-MHC-restricted cytotoxicity 1_6. TCR-dependant activation…. as well as TCR-independent stimulation….revealed the potential of peripheral T cells to behave as NK cells by switching to a non-MHC-restricted cytotoxicity pattern 6_9…..Common features of non-MHC-restricted T cells include their polyclonal activation via cytokine receptor triggering, the production of various cytokines and their non-MHC-restricted cytotoxicity. Recent evidence suggests the presence of NK-like cells in vivo in the gut of celiac patients….These CTL attacked autologous intestinal epithelial cells in a non-MHC-restricted fashion 13_14.”
von Geldern et. al. go on to describe their methodology and show how CD4+ and CD8+ cells can be ‘turned’ from passive to toxic without CD56 phenotyping, stating:
“CD56 was not found on CD4+ or CD8+ T cells” (pg 2354),
but that cytokine stimulation can induce a pattern of T cell phenotyping which is independent of antigen exposure, and that:
“non-MHC-restricted cytolytic pattern is strikingly similar to NK cell activity”.
Transmuting these results into the parameters exhibited in Table 5, we find the pattern of stimulation >> dysregulation to be confirmed. A vaccine was injected twice. Two severe reactions followed after each inoculation, the second leading to serious injury. The adjuvant or viral component (or both), shocked the liver into an apoptotic cascade, while also inducing the secretion of excessive amounts of cytokines. Massive releases of liver enzymes ensued, accompanied by large increases in WBC’s. After the ‘dust’ settled, the production of activated receptors (AR) failed to switch off due to the lingering effects of adjuvation or mimicry (or both), while sufficient numbers of inhibitory receptors (IR) which function to counter such increases, could not respond. Thus, after the initial shock, the immune system fell into a condition where it could no longer abrogate aggressive phenotypes that exceed system protocols. The persisting elevated NK and unrestricted T cell phenotypes in Table 5 mirror that breakdown in immune regulation. This entire process is a picture of dysregulation, where the immune system still functions but some of its protocols remain impaired.
What the experimental stimulation employed by immunotherapists shows is that:
Ø Researchers admit to inducing cytotoxic changes in undisturbed immune cells.
Ø Immune responses can occur outside of antigen-dependant safety protocols.
Ø Activated cytokine protocols can lead to unfavourable NK and T cell responses.
Ø Such activation can lead to toxic concentrations of aggressive phenotypes.
Ø CD56 phenotypes are not the only type of autoimmune cytotoxicity states.
Ø Normal MHC-restricted T cells can be transformed into NK-like T cells, ie: restricted T cells are ‘turned’ into non-restricted’ cells, with free aggression.
Ø Experiments are designed with the goal of inducing potent therapeutic remedies.
Ø “occasional high but variable and unpredictable clinical responses 39_42” do occur (von Geldern et.al. 2006, 2359).
Ø Researchers are aware that manipulation of the immune system can produce unpredictable and out-of-control autoimmune cytotoxicity.
What all this confirms is that the immune system is not some ethereal system that has a lifetime warranty and remains impervious to change, as vaccine campaigners hope. The truth is exactly the opposite. The immune system is easily shifted with often detrimental results, leading to damage that is often irreversible. The mass corruption of immune systems that we have seen in modern times can only be attributed to the mass deployment of immune stimulation devices – vaccines. This injurious process is not a new revelation by any means – researchers have known of the susceptibility of the immune system to manipulation for decades.
Thus, modern gene expression studies are revealing a picture of immune function impairment involving artificially shifted immune responses, cytolytic changes to beneficial protector cells, breakdowns in friendly recognition procedures, lysidic invasion of CD56 and other aggressive phenotypes, and resultant chronic injury states inflicted on unsuspecting recipients. In short, certain immune defenses that were once protective of their hosts, are converted by vaccine interference into hostile factions, which then not only combat traditional pathogens but also turn on their own hosts because they cannot switch off. The link between the author’s excessive compliment of cytotoxic phenotypes and the findings of the above researchers, strongly suggests a causal relationship between phenotypic activation and the author’s symptoms of injury. This cytotoxic link may be framed as follows:
· Total numbers of CD56 cytotoxic phenotypes are elevated, as Table 5 shows.
· NK cell activity for the author was highest in the group of seven test subjects.
· No pathogens or pre-existing conditions could be identified from the serology.
· No pathogenic justification exists therefore, for an increase in CD56 ranks.
· The action of vaccine stimulation is the only event in the author’s clinical history that could have induced such phenotypic conversion.
· The increased CD56’s must have target zones, otherwise why have such numbers?
· The target orientation of the immune defenses may now have changed.
· The author’s symptom states strongly identifies the new source of targeting.
· 15 body systems were disrupted soon after vaccination, with 12 remaining chronic.
· Marginal increases in the test group’s CD56 expression, appear to be sufficient to cause major disruption to health.
· Abnormal differentiation in other B cell, T cell, and NK cell lines might also contribute to injury states, such as CD 16 and CD 4 cytotoxic phenotypes.
· Out-of-control genetic self-targeting constitutes classic autoimmune injury.
These unnatural program changes therefore represent a dysregulation of inherited operational arrangements and may include any of the following mechanisms and outcomes:
Þ DNA base modifications, strand fragmentations, or portional recodes.
Þ Changes to existing histocompatibility arrangements.
Þ Changes to cell transport pathways, including faulty signaling.
Þ Alterations in protein specificities within or between cell lineages (eg: myeloid cells), due to the introduction of foreign peptides or modified proteins.
Þ Changes in friendly recognition resulting in death by mimickry.
Þ Shifts in cytokine and receptor balances causing excesses or deficiencies.
Þ Unnaturally high concentrations of aggressive cell phenotypes.
Þ Lysis of beneficial bacteria and/or mucosal barriers in the GIT.
Þ Lysis of mitochondria resulting in mass cell death (ie: apoptotic cascade).
Þ Impaired Krebs Cycle / impaired Methylation Cycle.
All of these injurious processes lead to chronic injury states such as Chronic Fatigue, Multiple Sclerosis, Irritable Bowel, and many other neurological and metabolic states.
iii): Author’s CFS Correlation:
The author was invited to participate in a Chronic Fatigue Syndrome (CFS) university case control study, which included serology investigations into the WBC immune subpopulations of a small group of CFS sufferer’s. Seven members of this group of about 200 people were regarded by the faculty staff as being severely impaired, including the author. The immune cell subpopulations under investigation included lymphocyte surface marker examination. The testing was undertaken to determine how sufferers of chronic fatigue differed immunologically from individuals of normal health. After the case study concluded, the author continued testing for irregularities within lymphocyte lineages including B cell, T cell, and NK cell sub-populations. The findings of these autoimmune markers are shown in Table 3, and have been discussed in greater detail in the previous subdivision relating to Table 5.
When Gherardi (2003) investigated autoimmune states as possible manifestations of vaccination sensitization in France, Gherardi described artificially shifted immune responses forming chronic fatigue syndromes, caused by aluminium adjuvants in certain vaccines. Other gene expression studies have also described shifted immunogenic responses giving credence to the growing body of evidence that vaccine damage is correctly a pathogenetic concept. Similar to Gherardi’s revelations, Nancy and Shoenfeld (2008) also implicated the onset of CFS in a patient in their study. They stated: “CFS etiology is multi-factorial commonly triggered by infectious agents. Vaccines, induce an immune response similarly to infections, and may trigger just like infections autoimmune diseases, CFS and fibromyalgia. Furthermore vaccines contain an adjuvant which enhances their immune stimulation …..Our patient illness started following hepatitis-B vaccine, suggesting that it was caused or accelerated by vaccination.”
The pathological immune stimulation Gherardi and other researchers have alerted to, involves alterations to the behavior of some lymphocyte lines rendering them with new aggressive expression towards their siblings and neighbours. As previously described, lineages in the Adaptive immune system evolve under chemo-genetic intervention into new activated phenotypes that infiltrate tissues, organs and pathways causing damage – an auto-immune coup` in other words. The resulting damage from such intervention is the development of neurological and inflammatory disease states such as CFS, GBS, MMF, MND, MS, and SLE; etc.
CFS has been the subject of many studies, including the university study noted above which the author participated in. CFS is clinically characterized by persistent and debilitating fatigue (ie: weakness and loss of stamina), which is not remedied by adequate rest, nutrition and sleep. The condition impairs daily activity and diminishes quality of life indefinitely in victims. Other CFS symptoms include headaches, dizziness, GIT disturbances, muscle pain, joint pain without the swelling, exercise penalty malaise, tender lymph nodes, and cognitive dysfunction such as impaired concentration, memory, mood and sleep.
The laboratory characterisation for CFS has remained elusive because repeatable biochemical markers have been unattainable or inconsistent, leaving diagnosis dependent primarily upon persisting clinical symptoms specific to each individual. In the body of literature investigating the causes of CFS, there are a variety of markers that although not consistent in all cases, do point to causal mechanisms. A list of these potential markers is compiled in Table 6 where comparison is made to the author’s empirical and clinical history. The lack of infectious triggers noted in Table 6 for the author’s CFS, has already been discussed in earlier sections.
As the author’s injury includes the primary symptoms of CFS, it would be logical to expect that some of these markers might be relevant to the author’s case. However, while some of these markers are still in the hypothetical stage, and other markers have not yet been tested in the author’s investigations, presently only three markers exhibit a point of contact with the author’s case history, those being:
- CFS preceded by vaccination (ie: vaccination caused CFS onset)
- Decreased serum Coenzyme Q10 (the energy molecule)
- Mitochondrial degeneration (associated with post-vaccination Liver Toxemia).
Thus, the etiology of synthetically induced CFS via a vaccine mechanism, is significantly more plausible than an infectious etiology, and supported by the positive correlation with the literature markers for post-vaccination onset and chronic liver toxemia.
Table 6 ……………………………………………………………………. > /
Table 6: Potential markers for CFS activation compared to the Author’s case.
.
Potential Markers l Author’s Medical Case
l .
CAUSAL MARKERS:
CFS onset preceded by new virus Last virus 18 months before injury
CFS onset by reactivated old virus No reactivation in serology or period.
CFS preceded by bacterial infection No bacterial infection in serology
CFS preceded by vaccination Yes – following HBV inoculation
BIOLOGICAL MARKERS:
Increased serum CRP CRP constantly normal
Decreased serum NK cells NK cells chronically elevated
Activation of CD 26, 38, 69 T cells None noted –only CD 56 elevated
Elevated serum auto-antibodies ANA, AAM, ANC, DNAA normal
Elevated B Cell phenotypes CD19 B Cells normal
Elevated pro-inflammatory cytokines Cytokine tests ordered >>
Decreased anti-inflammatory cytokines >> Results not supplied
Degranulation of T and NK Cells Untested
Excessive gut hydrogen sulfide (H2S) Untested
Elevated aerobic bacteria in GIT Untested
Elevated LPS for g.n. enterobacteria Untested
Depletion of antioxidants (L-glut./ 8-OHdG) Untested
Elevated serum lactic acid Untested
Decreased serum CoQ10 Yes – significant decrease
Activation of Mast Cells Untested
Mitochondrial degeneration Yes – in Liver Toxemia
Neural Inflammation CSF – IgG negative
iv): Author’s MS Correlation:
The chronic inability to maintain standing or walking for regular durations, together with the diffuse myalgias/dizziness/fatigue/GIT syndrome that the author has endured following HBV inoculations, strongly resembles MS-like autoimmune cytotoxicity even though limited specific serology for MS could not provide positive results. Parallel MS-like states however, without supporting MS pathology are known clinical manifestations for a variety of vaccines, and many vaccine injury reports similarly testify of ‘leg weakness’ and other neurological disorders. Numerous hospital corridors and waiting rooms have been influxed by vaccinated people who have found themselves in sudden and unexpected need of leg braces and wheelie walkers.
Hernan et.al. (2004) noted in their independent UK case control study:
“The OR (odds ratio) of MS for vaccination within 3 years before the index date compared to no vaccination was 3:1…..These findings are consistent with the hypothesis that immunization with the recombinant hepatitis B vaccine is associated with an increased risk of MS….” Mikaeloff et. al. 2009 also noted in their case control study of vaccinated French victims suffering similar neural demyelination between 1994-98; that “the Engerix B vaccine appears to increase this risk, particularly for confirmed multiple sclerosis, in the longer term.”
Girard (2005), who was privy to suppressed surveillance data arising from his consultancy background, stated: “In 25 years of professional life devoted to the study of drug hazards, I have rarely seen an issue clearer than that related to the potential of hepatitis B vaccine to induce auto-immune diseases.” Girard (2007) illustrated the link between the increase of MS states in France after 1994, and the deployment of HBV inoculations. Referring to the French vaccination campaign, he stated:
“Another observation of indisputable significance in post-marketing surveillance was a sharp increase in a disease (MS) whose spontaneous occurrence was miniscule before the introduction of the suspected vaccine…..this dramatic 25-fold increase during a period where mass vaccination against hepatitis B was the most drastic change in the health environment gives enormous credibility to the hypothesis of neurotoxicity linked to this vaccine…..this means that a number of doctors…..had never, in their professional lives, met a patient with MS. Nowadays however, at all social or professional levels, anybody – health professional or not knows of several cases of MS in people around him/her.”
MS and MS-like injuries are devastating conditions to acquire, and usually produce a constellation of symptoms. Authier et. al. (2001, 975) stated:
“The association between MMF and multiple sclerosis-like disorders may give new insights into the controversial issues surrounding vaccinations and demyelinating CNS disorders”.
A compilation of the more common MS symptoms has been listed below in Table 7. The 36 symptoms are commonly found on the major MS websites, and these are correlated to the author’s injury in terms of their phase occurrences and repetition.
iv): Author’s MS Correlation:
The chronic inability to maintain standing or walking for regular durations, together with the diffuse myalgias/dizziness/fatigue/GIT syndrome that the author has endured following HBV inoculations, strongly resembles MS-like autoimmune cytotoxicity even though limited specific serology for MS could not provide positive results. Parallel MS-like states however, without supporting MS pathology are known clinical manifestations for a variety of vaccines, and many vaccine injury reports similarly testify of ‘leg weakness’ and other neurological disorders. Numerous hospital corridors and waiting rooms have been influxed by vaccinated people who have found themselves in sudden and unexpected need of leg braces and wheelie walkers.
Hernan et.al. (2004) noted in their independent UK case control study:
“The OR (odds ratio) of MS for vaccination within 3 years before the index date compared to no vaccination was 3:1…..These findings are consistent with the hypothesis that immunization with the recombinant hepatitis B vaccine is associated with an increased risk of MS….” Mikaeloff et. al. 2009 also noted in their case control study of vaccinated French victims suffering similar neural demyelination between 1994-98; that “the Engerix B vaccine appears to increase this risk, particularly for confirmed multiple sclerosis, in the longer term.”
Girard (2005), who was privy to suppressed surveillance data arising from his consultancy background, stated: “In 25 years of professional life devoted to the study of drug hazards, I have rarely seen an issue clearer than that related to the potential of hepatitis B vaccine to induce auto-immune diseases.” Girard (2007) illustrated the link between the increase of MS states in France after 1994, and the deployment of HBV inoculations. Referring to the French vaccination campaign, he stated:
“Another observation of indisputable significance in post-marketing surveillance was a sharp increase in a disease (MS) whose spontaneous occurrence was miniscule before the introduction of the suspected vaccine…..this dramatic 25-fold increase during a period where mass vaccination against hepatitis B was the most drastic change in the health environment gives enormous credibility to the hypothesis of neurotoxicity linked to this vaccine…..this means that a number of doctors…..had never, in their professional lives, met a patient with MS. Nowadays however, at all social or professional levels, anybody – health professional or not knows of several cases of MS in people around him/her.”
MS and MS-like injuries are devastating conditions to acquire, and usually produce a constellation of symptoms. Authier et. al. (2001, 975) stated:
“The association between MMF and multiple sclerosis-like disorders may give new insights into the controversial issues surrounding vaccinations and demyelinating CNS disorders”.
A compilation of the more common MS symptoms has been listed below in Table 7. The 36 symptoms are commonly found on the major MS websites, and these are correlated to the author’s injury in terms of their phase occurrences and repetition.
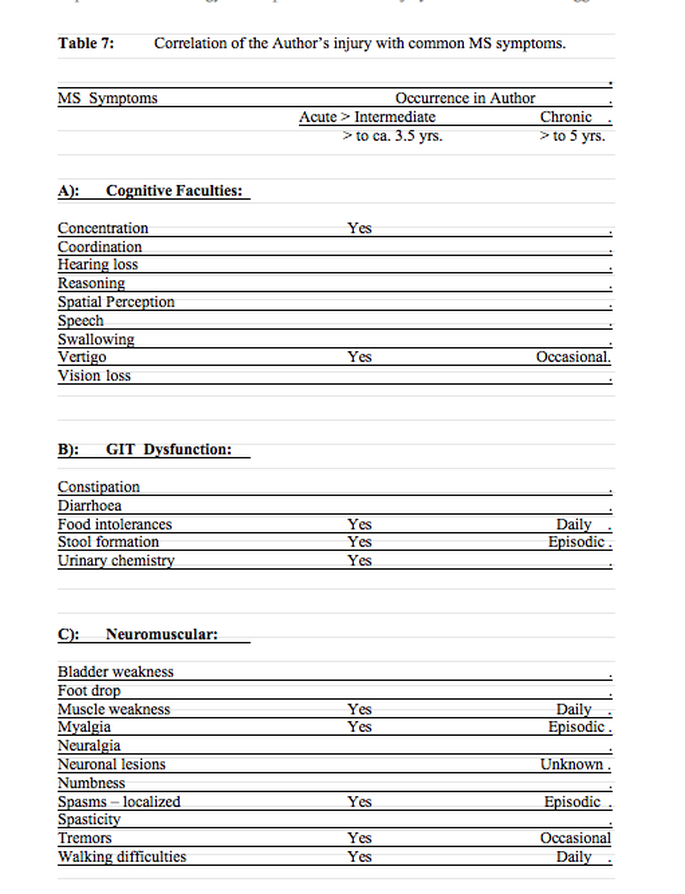
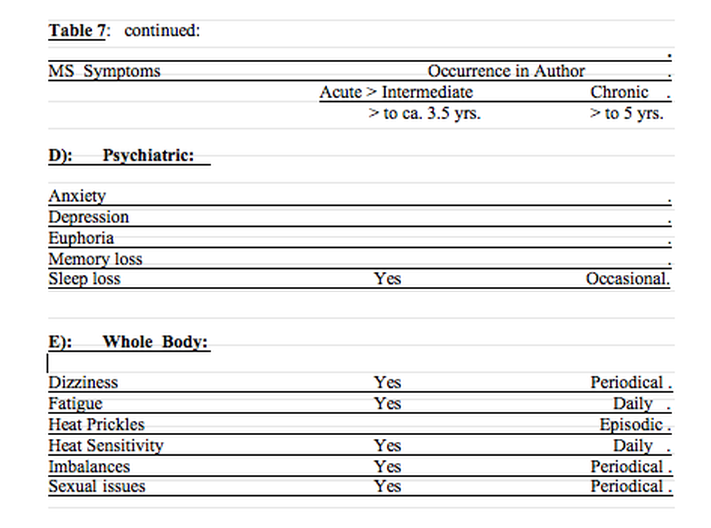
Many of these symptoms will vary widely in degree, pattern, and frequency between sufferers. Many suffers will only experience a small number of these symptoms. Neurological impairment is a common denominator in sufferers due to autoimmune cytotoxicity, with neural lesions being the trigger for some symptoms. Individual specificity suggests the impairment reaches down to the genetic level.
MS shares a cross-over relationship with other neurological diseases such as Autism, Devic’s Syndrome (DS), Chronic Inflammatory Demyelinating Polyneuropathy (CIDP), Chronic Fatigue Syndrome (CFS), Guillaine-barre Syndrome (GBS), Macrophagic Myofasciitis (MMF), Motor Neuron disease (MND), and Systemic Lupus Erythematosus (SLE). A number of neurological symptoms are shared by these diseases. Diagnosis may be based upon the highest cluster of symptoms in the sufferer, or upon changing medical definitions, or both. The link between vaccine toxicity and these diseases is sinister.
Diagnosis for MS using pathology investigations and clinical findings has been the subject of much debate, review and opposition; especially when the incidence of MS saw a parallel increase in countries such as France (Girard, 2007) with the widespread use of vaccines. MS diagnoses therefore have attached potential legal ramifications and payouts, prompting authorities to take note and develop liability-reducing strategies. In some countries for example, serum testing for MS is under the tight control of government agencies, where serology tests are automatically sent to government hospitals, rather than being performed by commercial labs.
Since the mid 1960’s when criteria for MS were first formulated, the debate has generally been polarized between whether MS is a pathologically-defined disease or a clinically-defined one. Some groups on the pathology side, argue that MS can only be proved by autopsy, or in some circumstances by biopsy. In 2001 McDonald et. al. revised earlier criteria, and argued that clinical manifestations were sufficient as grounds for an MS diagnosis. However, the McDonald criteria were soon challenged with two revisions, resulting in the final 2010 criteria (Polman et. al. 2011) which demanded that MRI evidence be awarded greater importance in MS diagnoses. Thus, the trend towards a pathological definition would automatically eliminate a significant number of existing diagnoses and reduce the number of future diagnoses. This is potentially problematic for sufferers who exhibit typical MS clinical symptoms, but whose MRI images do not reveal supporting evidence. It is problematic because primary progression of MS may last 10 years before lesions will show up on an MRI scan, placing convenient distance in time and space between causation and diagnosis, while also delaying and/or canceling victim’s compensation prospects.
Official diagnosis of MS is traditionally the monopoly of neurologists, although with modern scanning technology other specialists and GP’s could reliably develop the same diagnosis, thus eliminating the need for expensive neurology consultations. Many vaccine victims however, have reported neurologists being unwilling to assist victims in their diagnosis or treatment, in flagrant violation of Hippocratic loyalty. Given that systemic vaccine injuries frequently induce neurological states, reluctance on the part of neurologists is a foregone conclusion, since many neurologists do not wish to be seen to blacken the reputation of vaccines – and expect to remain in practice. This same reluctance was encountered by the author when approaching immunologists for medical reports. None of these were willing to get involved in the author’s case also. Patients soon discover that MS diagnoses are unpopular in some spheres of medicine, just as CFS was in the past – and still is in some quarters.
In the author’s case, having now waited some 5 years, a cerebral MRI is planned for the near future (health permitting), to ascertain if plaques or lesions have developed on the brain. Regardless whether these will be evident on the scans or not, a significant convergence of symptoms towards an MS-like profile has existed in the author following vaccination. Of the 36 clinical MS symptoms provided in Table 7, the author has experienced 16 after vaccination, representing an arbitrary share of 44% MS correlation. Of these 16, there are 14 chronic symptoms (either daily / episodic / periodical / or occasional), representing a 39% persistence correlation.
Despite negative serology results reported by labs for Neuronal Antibodies and Cerebral Spinal Fluid Immunoglobulin G tests, the remission / relapse cycle of some symptoms in Table 7 (particularly dizziness and localized spasms), could suggest disorder associated with central demyelinating disease. At this point in time a definite MS diagnosis has not been determined, and the author’s most severe symptoms may be wholly due to a damaged liver. However, the 39% persistence correlation from Table 7 would demonstrate that the author has a vaccine mediated parallel MS-like state as part of his constellation illness. Considering that sufferers who qualify as MS patients, may experience only a small number of symptoms from the compilation in Table 7, the current 39% correlation is evocative.
v): Warnings of Hepatitis B Vaccine (HBV) Toxicity:
The constellation of symptoms described in this report mirror the frequent systemic reactions generated by HBV’s worldwide. In fact, injuries from this vaccine are so alarming so as to cause an entire American medical collective to take a stand by speaking out against HBV toxicity and forced vaccine mandates. That collective is the AAPS (Association of American Physicians and Surgeons Inc.), a respected medical fraternity numbering some 5,000 doctors, whose headquarters are located in Tucsan, Arizona USA. The AAPS openly presents a united opposition against HBV’s, based on its recognition of this vaccine’s potential in particular for frequent and severe side-effects, as is demonstrated by the author’s symptoms.
The AAPS (2000) warned of the following: “Members of the….AAPS voted this week at their 57th Annual Meeting….to pass a resolution calling for an end to mandatory childhood vaccines. The resolution was passed without a single “no” vote…..Our children face the possibility of death or serious long-term adverse effects from mandated vaccines that aren’t necessary or that have very limited benefits…..children under the age of 14 are three times more likely to suffer adverse effects – including death – following the hepatitis b vaccine than to catch the disease itself…..students….. were sent home from school, and told they could not return until they had been forced to receive hep b vaccinations. Further, parents were threatened by Child Protection Services with possible seizure of their children based on ‘education neglect’”.
Maniotis et.al. (2006) remonstrated the frightening dangers of HBV’s in their important editorial, which in association with the AAPS (2004) was presented in abridged form before the Cook County Board of Commissioners on March 10, 2004. Maniotis et.al. warned:
“Some of the severe adverse effects include autism, Stevens-Johnson syndrome, arthritis both transient and permanent, Guillaine-Barre Syndrome, myelitis including transverse myelitis, seizure, febrile seizure, peripheral neuropathy including Bell’s palsy, diabetes mellitus, pancreatitis encephalitis, multiple sclerosis, thrombocytopenia, systemic lupus erythematosus, lupus-like syndrome, vasculitis, optic neuritis, radiculopathy. Lesser vaccine effects include vomiting, abdominal pains, vertigo, dizziness, pruritis, angioderma, urticaria, lymphadenopathy, insomnia, dysuria, hypotension, increased risk of shingles, migraine, severe muscle pain and weakness, hypesthesia, alopecia, petechiae, increased sedimentation rate, tinnitus, conjunctivitis, visual disturbances, syncope, tachycardia, keratitis, irritability [2].”
“The practical and economic impact of the effects of this mandated recombinant hepatitis B vaccine policy is devastating infants, families, and the nation, because the nature and frequency of the vaccine damage is typically so debilitating…… abundant evidence accumulated by the VAERS and the CDC shows that the hepatitis B vaccine is strongly associated with an unacceptable frequency of debilitating life long illnesses.”
.
The unusual increase in MS and parallel states in Europe and North America following vaccination drives, set in motion a barrage of immunogenic studies to determine the veracity of anecdotal claims of vaccine toxicity. By the end of 2001 there were over 110 research papers on HBV’s alone. Some were sponsored by industrialists and governments to appease public concerns, which usually found no dangers associated with these vaccines; while other studies were independently funded by separate research groups and which usually found there were significant dangers. The smell of protection racketeering verses the scent of credible science emanating from the vaccination literature has clearly polarized research articles, producing an academic war of philosophy between divided campaigners.
France is one of the first countries in the world to be subjected to heavy exposure to aluminium-containing vaccines such as HBV’s. France’s exposure has not only seen the rise of vaccine-mediated MS upon it’s gene pool, but also the rise of a new disease called macrophagic myofasciitis (MMF). Emerging in 1993, MMF was a new type of inflammatory myopathy with clinical manifestations of CFS states and diffuse muscle pain and joint pain, as noted earlier in this report. Gherardi (2003, 162) and other researchers have attributed the disease to aluminium adjuvants added to vaccines. By 2003, Gherardi noted there were some 200 definite cases of MMF in France, and the disease was also occurring in other European countries as well. Many of these cases were documented by an expert group of myopathologists at the Association Francaise Contre les Myopathies (Authier et.al. 2001, 975). The rate of MMF detection in one group of 113 vaccinated patients over a 1 year period, was noted by Gherardi et.al. (2001) to be 13%. Deltoid muscle biopsy of these patients found macrophages around injection sites were invaded by dark spicular bodies. Gherardi et.al. describes these aluminium-loaded macrophages as follows: “Inclusions appeared as aggregates of fine needle-shaped randomly oriented dense structures, forming clusters, often bounded by a distinct lysosomal membrane, in macrophages”. They also noted that “a lymphocytic component was constantly observed in MMF lesions”.
Thus, in July 1998 after 4 years of HBV inoculations had been imposed upon 30 million French citizens, the cytotoxic and neurological effects of HBV’s became so apparent, that the philosophical war moved into the courts. This included a notable class action against the French government involving some 15,000 claimants. Although court documentation is not readily available, trickle reports are noted in the journals – such as the successful compensation of two hospital workers, reported by deBousingen (2001, 1598), and the report noted by Marshall (1998, 650-1) below.
Marshall noted the following: “Already, several groups are seeking compensation from governments and manufacturers or demanding that mandatory vaccination be stopped. On 17 July, for example, an alliance of antivaccine activists in France filed for a lawsuit in Paris against the national government, accusing it of understating the vaccine’s risks and exaggerating the benefits for the average person. The attorneys, who seek a criminal inquiry, claim to represent 15,000 people. And in the United States, several East Coast lawyers representing clients with hepatitis vaccine claims held a summit near Washington, D.C., in July to discuss strategy…..Physician Philippe Jacubowicz, who heads an organization in Paris called REVAHB, has collected data on more than 600 cases of illnesses, many with MS-like symptoms, in people who had received the hepatitis B vaccine. In addition, patient advocacy groups in Britain and Canada have studied more than 100 cases each, as has an outspoken U.S. accuser of the hepatitis B vaccine, Bonnie Dunbar, a molecular biologist at Baylor College of Medicine in Houston.”
Further evidence for the public backlash in France is noted from the reluctant Federal suspension of the vaccine in October 1998 from schools for reasons of neurotoxic safety concerns, against howls of protests from pediatricians and others (Dorozynski 1998, 1034). The nation-wide terror also attracted the interest of Medscape (2002) who released some details of a critical report ordered by Judge Marie-Odile Bertella-Geffroy and prepared by Pharmacoepidemiologist and industry expert Dr. Marc Girard. In his report Girard noted that crucial evidence of vaccine tolerance was withheld from doctors so as not to ruin the vaccination drive, and that health authorities worked to minimize the situation after thousands of MS/neurological injuries had flooded in. The Medscape release also noted a memo from the French General Directorate for Health dated 15 February 2002, which stated that the hepatitis B campaign produced the “greatest series of side effects noted by Pharmacovigilance since its creation in 1974.”
Alarm over HBV’s has also prompted a number of doctors to publicly submit their own individual objections, declaring their findings on the internet or by preparing DVD’s, or by running public seminars or lodging official testimonies. For example, a posting by UK practitioner Charles Shepherd MD (2001) declared the following statistics from his clinical practice:
“My research interest in this aspect of developing CFS is largely based on clinical evidence from patients seen in my practice over the past 10 years. As a result, I have gathered details on more than 200 patients with a history of either developing CFS or experiencing a significant relapse / exacerbation of CFS symptoms following a vaccination….. This data (although unpublished) suggests that tetanus, typhoid, influenza, and hepatitis B are the most commonly implicated vaccines in cases of CFS…. Almost all of my cases involve adults……. About one third of my cases involve vaccine induced / exacerbated CFS following receiving the hepatitis B vaccine (HBV). Most of these patients are healthcare workers, particularly nurses. Most of the other patients received HBV for occupational health purposes….. The prognosis in this group has been poor, with less than 10% of the patients I have personally followed reporting any significant relief of CFS symptoms.
Another practitioner, Byron Hyde MD (circa 1996) from Canada, lodged his testimony before the Quebec College of Physicians Medical Board, saying:
“We looked at hep B immunisation in Quebec province because one nurse phoned us saying she had CFS after having hep B immunisation…..About a month later the same nurse called again, she now had 5 other nurses in the area who had fallen ill with CFS-like symptoms after the vaccine, all were unable to return to work…..This same nurse….(had) amassed 20 or 30 names of individuals, all post hep B immunisation cases…..We received close to 120 calls from nurses and health care workers in the Quebec area with problems…..many were disabled.”
HBV carnage also attracted the attention of a scientist of autoimmunity and vaccinology, namely Professor Bonnie S. Dunbar, whose own laboratory co-workers fell ill after HBV vaccination. In her 1999 report to the US House of Representatives she stated:
“About 5 years ago I had two individuals working in my laboratory who were required to take the Hepatitis B vaccine. Both of those individuals developed severe and apparently permanent adverse reactions as a result of the vaccine…….these two active, healthy individuals …..developed autoimmune syndromes within a predictable immunological timeframe following their booster injections of the hepatitis B vaccine….these adverse reactions are related to the nature of the viral protein, the recombinant surface antigen of which is the principal component of the vaccine.
I have been in contact with numerous physicians and research scientists from several countries who have independently described identical severe reactions to the vaccine in thousands of Caucasians. Their observations have been, for the most part, denied or ignored by the public health systems, as is evidenced by the serious charges against healthcare officials and pharmaceutical companies brought recently in France. The reversal of the vaccine mandate for children in France was not based on lack of documentation. I have now been contacted personally by hundreds or more individual’s…. who have reported deaths, severe health problems and life long disabilities resulting in major medical costs following the administration of this vaccine.”
Australian HBV statistics are showing similar patterns within our small population of some 24 million souls. Data provided from the Therapeutic Goods Administration (TGA) to the author in June 2012 showed since the first use of HBV’s in Australia in 1983, there were 4,689 adverse reports to 22.06.2012. In the period from 01.01.2009 to 22.06.2012 (180.86 weeks) – a period of 3.5 years – there were 1,791 adverse reports relating to vaccines containing the Hepatitis B antigen, equating to 9.90 adverse reports per week! Although this data includes adverse reports from one combination-vaccine containing other antigens for other diseases additional to the hepatitis B recombinant antigen, the total weekly reports still remain significantly alarming. Regrettably, and in violation of their Hippocratic oath, many of our doctors remain silent on this issue.
HBV’s, along with other known reactive vaccines such as DTP, MMR, Influenza mixtures, and HPV; are producing alarming injuries in populations, with future ramifications yet to be realized. When viewed in the context of herd health, gene pool instability and impairment, and the rise of vaccine-resistant diseases; the smug arrogance of vaccine campaigners have much to answer for.
Ø Part 4: OVERVIEW AT THE 5 YEAR MARKER.
At the 5 year marker (March 2014), daily liver discomfort or pain remains a regular pattern of the author’s illness. Abnormalities in liver enzymes took 3.5 years before finally settling. Neutrophil and lymphocyte subsets and episodic genital thrush also took 3.5 years to settle. All of the chronic symptoms listed in the “Chronology of Illness” summary (pg 9) continue to be present with the exception of insomnia and persisting back pain. Unfortunately, an intolerance to oral antibiotics was acquired through this injury, demonstrated by rapid pulse and giddiness after exposure to small amounts of penicillin class drugs.
The impaired digestive function reported in this study is evocative of a lowered immune performance, given that the primary sphere of immune capacity resides in the gastrointestinal tract (GIT). The post inoculation intolerances to wheaten foods (pgs 47, 58), oral antibiotics, certain herb teas and canned foods; all point to digestive immune system damage. Reactions to amino acid supplement powders (recommended by some researchers for chronic fatigue), also demonstrates the reluctance of the GIT to receive by artificial delivery, ‘unlocked’ amino acids. Where before inoculation the GIT would tolerate imperfect and processed foodstuffs, this pre-vaccination digestive buffer that once existed and provided so much benefit, now appears removed during the process of injury attributable to vaccine-mediated immunogenic dysregulation.
The GIT commands as much as 80% of the entire body’s complement of immune cells, and this tract is dependant upon a symbiotic relationship with microbes in order to supply the body with fuel for energy. Any disturbances to the energy supply derived from that equilibrium can be catastrophic to digestive wellness and personal endurance. The damage can occur at the microbial level, the intercellular level (impaired mitochondria), the intracellular level (impaired cell transport or signaling), or at the DNA level – or a combination of these resulting in loss of stamina and the introduction of chronic weakness and degenerative neuromuscular states. Whichever process or combination occurs, the result is an artificially shifted immune mechanism in the GIT as well as in the bloodstream.
The overall diagnosis for the author’s injury is a mixed bag. The severe unrelenting fatigue is consistent with CFS while the reactive GIT and painful liver is consistent with IBS and liver toxemia, both being vaccine-induced injuries attributable to an aluminium hydroxide mechanism known to pathologically shift immune and cell programming, leading to chronic neuromuscular and metabolic disorders. Similarly, the broad symptom correlation in Table 7 also corresponds to a parallel MS-like state via mechanisms of genetic degradation or dysregulation. Given the constellation of symptoms and without further delineating pathology for neuromuscular lesions, a local clinician felt justified in diagnosing the whole injury as a ‘Post Hepatitis B Vaccination Reaction Syndrome’.
Table 8 below contains a compilation of the author’s adverse symptoms of injury following HBV inoculation, correlated to known human biological (body) systems. The adverse symptoms are graded according to their longevity, namely transient (acute), intermediate, or persisting (chronic). An arbitrary separation of symptoms is also given with Table 8, identified as ‘Phase Durations”.
MS shares a cross-over relationship with other neurological diseases such as Autism, Devic’s Syndrome (DS), Chronic Inflammatory Demyelinating Polyneuropathy (CIDP), Chronic Fatigue Syndrome (CFS), Guillaine-barre Syndrome (GBS), Macrophagic Myofasciitis (MMF), Motor Neuron disease (MND), and Systemic Lupus Erythematosus (SLE). A number of neurological symptoms are shared by these diseases. Diagnosis may be based upon the highest cluster of symptoms in the sufferer, or upon changing medical definitions, or both. The link between vaccine toxicity and these diseases is sinister.
Diagnosis for MS using pathology investigations and clinical findings has been the subject of much debate, review and opposition; especially when the incidence of MS saw a parallel increase in countries such as France (Girard, 2007) with the widespread use of vaccines. MS diagnoses therefore have attached potential legal ramifications and payouts, prompting authorities to take note and develop liability-reducing strategies. In some countries for example, serum testing for MS is under the tight control of government agencies, where serology tests are automatically sent to government hospitals, rather than being performed by commercial labs.
Since the mid 1960’s when criteria for MS were first formulated, the debate has generally been polarized between whether MS is a pathologically-defined disease or a clinically-defined one. Some groups on the pathology side, argue that MS can only be proved by autopsy, or in some circumstances by biopsy. In 2001 McDonald et. al. revised earlier criteria, and argued that clinical manifestations were sufficient as grounds for an MS diagnosis. However, the McDonald criteria were soon challenged with two revisions, resulting in the final 2010 criteria (Polman et. al. 2011) which demanded that MRI evidence be awarded greater importance in MS diagnoses. Thus, the trend towards a pathological definition would automatically eliminate a significant number of existing diagnoses and reduce the number of future diagnoses. This is potentially problematic for sufferers who exhibit typical MS clinical symptoms, but whose MRI images do not reveal supporting evidence. It is problematic because primary progression of MS may last 10 years before lesions will show up on an MRI scan, placing convenient distance in time and space between causation and diagnosis, while also delaying and/or canceling victim’s compensation prospects.
Official diagnosis of MS is traditionally the monopoly of neurologists, although with modern scanning technology other specialists and GP’s could reliably develop the same diagnosis, thus eliminating the need for expensive neurology consultations. Many vaccine victims however, have reported neurologists being unwilling to assist victims in their diagnosis or treatment, in flagrant violation of Hippocratic loyalty. Given that systemic vaccine injuries frequently induce neurological states, reluctance on the part of neurologists is a foregone conclusion, since many neurologists do not wish to be seen to blacken the reputation of vaccines – and expect to remain in practice. This same reluctance was encountered by the author when approaching immunologists for medical reports. None of these were willing to get involved in the author’s case also. Patients soon discover that MS diagnoses are unpopular in some spheres of medicine, just as CFS was in the past – and still is in some quarters.
In the author’s case, having now waited some 5 years, a cerebral MRI is planned for the near future (health permitting), to ascertain if plaques or lesions have developed on the brain. Regardless whether these will be evident on the scans or not, a significant convergence of symptoms towards an MS-like profile has existed in the author following vaccination. Of the 36 clinical MS symptoms provided in Table 7, the author has experienced 16 after vaccination, representing an arbitrary share of 44% MS correlation. Of these 16, there are 14 chronic symptoms (either daily / episodic / periodical / or occasional), representing a 39% persistence correlation.
Despite negative serology results reported by labs for Neuronal Antibodies and Cerebral Spinal Fluid Immunoglobulin G tests, the remission / relapse cycle of some symptoms in Table 7 (particularly dizziness and localized spasms), could suggest disorder associated with central demyelinating disease. At this point in time a definite MS diagnosis has not been determined, and the author’s most severe symptoms may be wholly due to a damaged liver. However, the 39% persistence correlation from Table 7 would demonstrate that the author has a vaccine mediated parallel MS-like state as part of his constellation illness. Considering that sufferers who qualify as MS patients, may experience only a small number of symptoms from the compilation in Table 7, the current 39% correlation is evocative.
v): Warnings of Hepatitis B Vaccine (HBV) Toxicity:
The constellation of symptoms described in this report mirror the frequent systemic reactions generated by HBV’s worldwide. In fact, injuries from this vaccine are so alarming so as to cause an entire American medical collective to take a stand by speaking out against HBV toxicity and forced vaccine mandates. That collective is the AAPS (Association of American Physicians and Surgeons Inc.), a respected medical fraternity numbering some 5,000 doctors, whose headquarters are located in Tucsan, Arizona USA. The AAPS openly presents a united opposition against HBV’s, based on its recognition of this vaccine’s potential in particular for frequent and severe side-effects, as is demonstrated by the author’s symptoms.
The AAPS (2000) warned of the following: “Members of the….AAPS voted this week at their 57th Annual Meeting….to pass a resolution calling for an end to mandatory childhood vaccines. The resolution was passed without a single “no” vote…..Our children face the possibility of death or serious long-term adverse effects from mandated vaccines that aren’t necessary or that have very limited benefits…..children under the age of 14 are three times more likely to suffer adverse effects – including death – following the hepatitis b vaccine than to catch the disease itself…..students….. were sent home from school, and told they could not return until they had been forced to receive hep b vaccinations. Further, parents were threatened by Child Protection Services with possible seizure of their children based on ‘education neglect’”.
Maniotis et.al. (2006) remonstrated the frightening dangers of HBV’s in their important editorial, which in association with the AAPS (2004) was presented in abridged form before the Cook County Board of Commissioners on March 10, 2004. Maniotis et.al. warned:
“Some of the severe adverse effects include autism, Stevens-Johnson syndrome, arthritis both transient and permanent, Guillaine-Barre Syndrome, myelitis including transverse myelitis, seizure, febrile seizure, peripheral neuropathy including Bell’s palsy, diabetes mellitus, pancreatitis encephalitis, multiple sclerosis, thrombocytopenia, systemic lupus erythematosus, lupus-like syndrome, vasculitis, optic neuritis, radiculopathy. Lesser vaccine effects include vomiting, abdominal pains, vertigo, dizziness, pruritis, angioderma, urticaria, lymphadenopathy, insomnia, dysuria, hypotension, increased risk of shingles, migraine, severe muscle pain and weakness, hypesthesia, alopecia, petechiae, increased sedimentation rate, tinnitus, conjunctivitis, visual disturbances, syncope, tachycardia, keratitis, irritability [2].”
“The practical and economic impact of the effects of this mandated recombinant hepatitis B vaccine policy is devastating infants, families, and the nation, because the nature and frequency of the vaccine damage is typically so debilitating…… abundant evidence accumulated by the VAERS and the CDC shows that the hepatitis B vaccine is strongly associated with an unacceptable frequency of debilitating life long illnesses.”
.
The unusual increase in MS and parallel states in Europe and North America following vaccination drives, set in motion a barrage of immunogenic studies to determine the veracity of anecdotal claims of vaccine toxicity. By the end of 2001 there were over 110 research papers on HBV’s alone. Some were sponsored by industrialists and governments to appease public concerns, which usually found no dangers associated with these vaccines; while other studies were independently funded by separate research groups and which usually found there were significant dangers. The smell of protection racketeering verses the scent of credible science emanating from the vaccination literature has clearly polarized research articles, producing an academic war of philosophy between divided campaigners.
France is one of the first countries in the world to be subjected to heavy exposure to aluminium-containing vaccines such as HBV’s. France’s exposure has not only seen the rise of vaccine-mediated MS upon it’s gene pool, but also the rise of a new disease called macrophagic myofasciitis (MMF). Emerging in 1993, MMF was a new type of inflammatory myopathy with clinical manifestations of CFS states and diffuse muscle pain and joint pain, as noted earlier in this report. Gherardi (2003, 162) and other researchers have attributed the disease to aluminium adjuvants added to vaccines. By 2003, Gherardi noted there were some 200 definite cases of MMF in France, and the disease was also occurring in other European countries as well. Many of these cases were documented by an expert group of myopathologists at the Association Francaise Contre les Myopathies (Authier et.al. 2001, 975). The rate of MMF detection in one group of 113 vaccinated patients over a 1 year period, was noted by Gherardi et.al. (2001) to be 13%. Deltoid muscle biopsy of these patients found macrophages around injection sites were invaded by dark spicular bodies. Gherardi et.al. describes these aluminium-loaded macrophages as follows: “Inclusions appeared as aggregates of fine needle-shaped randomly oriented dense structures, forming clusters, often bounded by a distinct lysosomal membrane, in macrophages”. They also noted that “a lymphocytic component was constantly observed in MMF lesions”.
Thus, in July 1998 after 4 years of HBV inoculations had been imposed upon 30 million French citizens, the cytotoxic and neurological effects of HBV’s became so apparent, that the philosophical war moved into the courts. This included a notable class action against the French government involving some 15,000 claimants. Although court documentation is not readily available, trickle reports are noted in the journals – such as the successful compensation of two hospital workers, reported by deBousingen (2001, 1598), and the report noted by Marshall (1998, 650-1) below.
Marshall noted the following: “Already, several groups are seeking compensation from governments and manufacturers or demanding that mandatory vaccination be stopped. On 17 July, for example, an alliance of antivaccine activists in France filed for a lawsuit in Paris against the national government, accusing it of understating the vaccine’s risks and exaggerating the benefits for the average person. The attorneys, who seek a criminal inquiry, claim to represent 15,000 people. And in the United States, several East Coast lawyers representing clients with hepatitis vaccine claims held a summit near Washington, D.C., in July to discuss strategy…..Physician Philippe Jacubowicz, who heads an organization in Paris called REVAHB, has collected data on more than 600 cases of illnesses, many with MS-like symptoms, in people who had received the hepatitis B vaccine. In addition, patient advocacy groups in Britain and Canada have studied more than 100 cases each, as has an outspoken U.S. accuser of the hepatitis B vaccine, Bonnie Dunbar, a molecular biologist at Baylor College of Medicine in Houston.”
Further evidence for the public backlash in France is noted from the reluctant Federal suspension of the vaccine in October 1998 from schools for reasons of neurotoxic safety concerns, against howls of protests from pediatricians and others (Dorozynski 1998, 1034). The nation-wide terror also attracted the interest of Medscape (2002) who released some details of a critical report ordered by Judge Marie-Odile Bertella-Geffroy and prepared by Pharmacoepidemiologist and industry expert Dr. Marc Girard. In his report Girard noted that crucial evidence of vaccine tolerance was withheld from doctors so as not to ruin the vaccination drive, and that health authorities worked to minimize the situation after thousands of MS/neurological injuries had flooded in. The Medscape release also noted a memo from the French General Directorate for Health dated 15 February 2002, which stated that the hepatitis B campaign produced the “greatest series of side effects noted by Pharmacovigilance since its creation in 1974.”
Alarm over HBV’s has also prompted a number of doctors to publicly submit their own individual objections, declaring their findings on the internet or by preparing DVD’s, or by running public seminars or lodging official testimonies. For example, a posting by UK practitioner Charles Shepherd MD (2001) declared the following statistics from his clinical practice:
“My research interest in this aspect of developing CFS is largely based on clinical evidence from patients seen in my practice over the past 10 years. As a result, I have gathered details on more than 200 patients with a history of either developing CFS or experiencing a significant relapse / exacerbation of CFS symptoms following a vaccination….. This data (although unpublished) suggests that tetanus, typhoid, influenza, and hepatitis B are the most commonly implicated vaccines in cases of CFS…. Almost all of my cases involve adults……. About one third of my cases involve vaccine induced / exacerbated CFS following receiving the hepatitis B vaccine (HBV). Most of these patients are healthcare workers, particularly nurses. Most of the other patients received HBV for occupational health purposes….. The prognosis in this group has been poor, with less than 10% of the patients I have personally followed reporting any significant relief of CFS symptoms.
Another practitioner, Byron Hyde MD (circa 1996) from Canada, lodged his testimony before the Quebec College of Physicians Medical Board, saying:
“We looked at hep B immunisation in Quebec province because one nurse phoned us saying she had CFS after having hep B immunisation…..About a month later the same nurse called again, she now had 5 other nurses in the area who had fallen ill with CFS-like symptoms after the vaccine, all were unable to return to work…..This same nurse….(had) amassed 20 or 30 names of individuals, all post hep B immunisation cases…..We received close to 120 calls from nurses and health care workers in the Quebec area with problems…..many were disabled.”
HBV carnage also attracted the attention of a scientist of autoimmunity and vaccinology, namely Professor Bonnie S. Dunbar, whose own laboratory co-workers fell ill after HBV vaccination. In her 1999 report to the US House of Representatives she stated:
“About 5 years ago I had two individuals working in my laboratory who were required to take the Hepatitis B vaccine. Both of those individuals developed severe and apparently permanent adverse reactions as a result of the vaccine…….these two active, healthy individuals …..developed autoimmune syndromes within a predictable immunological timeframe following their booster injections of the hepatitis B vaccine….these adverse reactions are related to the nature of the viral protein, the recombinant surface antigen of which is the principal component of the vaccine.
I have been in contact with numerous physicians and research scientists from several countries who have independently described identical severe reactions to the vaccine in thousands of Caucasians. Their observations have been, for the most part, denied or ignored by the public health systems, as is evidenced by the serious charges against healthcare officials and pharmaceutical companies brought recently in France. The reversal of the vaccine mandate for children in France was not based on lack of documentation. I have now been contacted personally by hundreds or more individual’s…. who have reported deaths, severe health problems and life long disabilities resulting in major medical costs following the administration of this vaccine.”
Australian HBV statistics are showing similar patterns within our small population of some 24 million souls. Data provided from the Therapeutic Goods Administration (TGA) to the author in June 2012 showed since the first use of HBV’s in Australia in 1983, there were 4,689 adverse reports to 22.06.2012. In the period from 01.01.2009 to 22.06.2012 (180.86 weeks) – a period of 3.5 years – there were 1,791 adverse reports relating to vaccines containing the Hepatitis B antigen, equating to 9.90 adverse reports per week! Although this data includes adverse reports from one combination-vaccine containing other antigens for other diseases additional to the hepatitis B recombinant antigen, the total weekly reports still remain significantly alarming. Regrettably, and in violation of their Hippocratic oath, many of our doctors remain silent on this issue.
HBV’s, along with other known reactive vaccines such as DTP, MMR, Influenza mixtures, and HPV; are producing alarming injuries in populations, with future ramifications yet to be realized. When viewed in the context of herd health, gene pool instability and impairment, and the rise of vaccine-resistant diseases; the smug arrogance of vaccine campaigners have much to answer for.
Ø Part 4: OVERVIEW AT THE 5 YEAR MARKER.
At the 5 year marker (March 2014), daily liver discomfort or pain remains a regular pattern of the author’s illness. Abnormalities in liver enzymes took 3.5 years before finally settling. Neutrophil and lymphocyte subsets and episodic genital thrush also took 3.5 years to settle. All of the chronic symptoms listed in the “Chronology of Illness” summary (pg 9) continue to be present with the exception of insomnia and persisting back pain. Unfortunately, an intolerance to oral antibiotics was acquired through this injury, demonstrated by rapid pulse and giddiness after exposure to small amounts of penicillin class drugs.
The impaired digestive function reported in this study is evocative of a lowered immune performance, given that the primary sphere of immune capacity resides in the gastrointestinal tract (GIT). The post inoculation intolerances to wheaten foods (pgs 47, 58), oral antibiotics, certain herb teas and canned foods; all point to digestive immune system damage. Reactions to amino acid supplement powders (recommended by some researchers for chronic fatigue), also demonstrates the reluctance of the GIT to receive by artificial delivery, ‘unlocked’ amino acids. Where before inoculation the GIT would tolerate imperfect and processed foodstuffs, this pre-vaccination digestive buffer that once existed and provided so much benefit, now appears removed during the process of injury attributable to vaccine-mediated immunogenic dysregulation.
The GIT commands as much as 80% of the entire body’s complement of immune cells, and this tract is dependant upon a symbiotic relationship with microbes in order to supply the body with fuel for energy. Any disturbances to the energy supply derived from that equilibrium can be catastrophic to digestive wellness and personal endurance. The damage can occur at the microbial level, the intercellular level (impaired mitochondria), the intracellular level (impaired cell transport or signaling), or at the DNA level – or a combination of these resulting in loss of stamina and the introduction of chronic weakness and degenerative neuromuscular states. Whichever process or combination occurs, the result is an artificially shifted immune mechanism in the GIT as well as in the bloodstream.
The overall diagnosis for the author’s injury is a mixed bag. The severe unrelenting fatigue is consistent with CFS while the reactive GIT and painful liver is consistent with IBS and liver toxemia, both being vaccine-induced injuries attributable to an aluminium hydroxide mechanism known to pathologically shift immune and cell programming, leading to chronic neuromuscular and metabolic disorders. Similarly, the broad symptom correlation in Table 7 also corresponds to a parallel MS-like state via mechanisms of genetic degradation or dysregulation. Given the constellation of symptoms and without further delineating pathology for neuromuscular lesions, a local clinician felt justified in diagnosing the whole injury as a ‘Post Hepatitis B Vaccination Reaction Syndrome’.
Table 8 below contains a compilation of the author’s adverse symptoms of injury following HBV inoculation, correlated to known human biological (body) systems. The adverse symptoms are graded according to their longevity, namely transient (acute), intermediate, or persisting (chronic). An arbitrary separation of symptoms is also given with Table 8, identified as ‘Phase Durations”.
F): CONCLUSION:
To summarise, our analysis has progressed through an extensive assortment of pathology investigations leading to one logical and validated finding, that the Hepatitis B vaccine was solely responsible for the author’s illness. Given that the vaccine is itself a foreign immunological agent, there is a strong correlation between this agent and the inflammatory immunological state the author suffered. The liver and lymphatic systems were strongly disrupted after receiving the vaccine, both these systems showing inflammation. The liver function tests showed enzyme irregularities persisting for 3.5 years after inoculation, indicating an adverse chemical disorder remaining long after the acute phase inflammations had subsided.
The WBC subpopulations showed similar disruption, including lymphocyte subsets which displayed chronic genetic stimulation. Thus, the vaccine is the only documented agent in the author’s clinical environment capable of causing severe functional distress to the liver, lymph, digestive, neuromuscular and energy systems. These functional defects correspond with the acknowledged side effects declared by the vaccine manufacturer, in their Product Information Leaflet (PIL).
The evidence herein does not rely upon theory or medical opinion, but relies upon the accumulated empirical findings derived from an exhaustive battery of tests correlated with clinical observations of symptom type, latency and duration. The data strongly excludes any live and contemporary infections given there were no active infectious agents that could be identified. The injury has persisted long after typical pathogenic life cycles run their course (of incubation > manifestation > and subsidence). Neither could any pre-existing conditions be identified. The evidence herein solely defines a unique relationship (or link) between the Hepatitis B vaccine and the author’s injury. It identifies the nature of the relationship, the timing of the relationship, and the duration of the relationship. The empirical findings of this study therefore contribute to the material facts surrounding the author’s injury.
Australian regulations state that a medical product must be proved safe, but it does not have to be proved effective. In the author’s case, the HBV received failed on both counts, as it has been demonstrated herein that this vaccine was both unsafe and ineffective! Since vaccines are immunogenic conditioners and manipulators of the genetic environment of their hosts, once a host’s immune system is genetically shifted to a new program, even a self-destructive program, the potential for those artificial changes to remain permanent are significant. Effective immunisation however, from such immune shifts is remote. Finding and replicating the immunogenic key that deactivates or switches off the new programming, without the repressive effects of suppression drugs, is a technology that lies decades away, if it is achievable at all.
Given that the expected immune markers for vaccine causation were fully supported by the empirical data and clinical observations, the proposition at the beginning of this investigation that a foreign immune agent (the vaccine) was entirely responsible for the author’s injury, is fully endorsed. The profile of this harmful relationship is identified as follows:
Profile of Vaccine Causal Link:
The clinical and empirical evidence demonstrates an eight-fold causal link between the Hepatitis B Vaccine and the author’s injury:
1): Negative screening results for pathogens and pre-existing conditions in the extensive serology testing, supports an exclusion diagnosis.
2): Two separate reactions characterised by a constellation of adverse symptoms, causing severe and chronic disruption to the author’s health.
3): The eruption of multiple immune inflammatory markers, namely:
Ø 80% increase in total White Blood Cell levels above the norm.
Ø 3.5 year alteration to neutrophil and lymphocyte cell ratios from the norm, and chronically elevated cytotoxic NK and non-MHCR cells.
Ø Enlargement of the liver lobes and lymph glands, with RHS abdominal pain, despite negative screening results for hepatic viremia.
Ø 300% serum increase in ALT Liver enzyme levels above the norm.
Ø Increases in body temperature (fever) for 2 days, then 22 days, at start of each respective reaction.
Ø Sudden onset of low grade leg paralysis, diffuse myalgias and fatigue.
4): The repeated latency of symptoms (of 22 and 21 days) after each inoculation, links each delay with each respective injection.
5): The recurrence of the same symptoms after re-exposure to the same drug (a Positive Rechallenge), with a marked increase in severity of the second adverse reaction.
6): The long phase distribution of immune disruption (as Acute, Intermediate, & Chronic phases), extending well past documented life cycle time-frames of viral and bacterial infections.
7): The post development of immune intolerances via the digestive pathway to oral antibiotics and certain foods, previously well tolerated. Acquired sensitivities and allergies are expressions of immune condition.
8): The correlation of the author’s adverse symptoms with the vaccine manufacturer’s declared side-effects, as published in their vaccine Product Information Leaflet (PIL).
P.T.
To summarise, our analysis has progressed through an extensive assortment of pathology investigations leading to one logical and validated finding, that the Hepatitis B vaccine was solely responsible for the author’s illness. Given that the vaccine is itself a foreign immunological agent, there is a strong correlation between this agent and the inflammatory immunological state the author suffered. The liver and lymphatic systems were strongly disrupted after receiving the vaccine, both these systems showing inflammation. The liver function tests showed enzyme irregularities persisting for 3.5 years after inoculation, indicating an adverse chemical disorder remaining long after the acute phase inflammations had subsided.
The WBC subpopulations showed similar disruption, including lymphocyte subsets which displayed chronic genetic stimulation. Thus, the vaccine is the only documented agent in the author’s clinical environment capable of causing severe functional distress to the liver, lymph, digestive, neuromuscular and energy systems. These functional defects correspond with the acknowledged side effects declared by the vaccine manufacturer, in their Product Information Leaflet (PIL).
The evidence herein does not rely upon theory or medical opinion, but relies upon the accumulated empirical findings derived from an exhaustive battery of tests correlated with clinical observations of symptom type, latency and duration. The data strongly excludes any live and contemporary infections given there were no active infectious agents that could be identified. The injury has persisted long after typical pathogenic life cycles run their course (of incubation > manifestation > and subsidence). Neither could any pre-existing conditions be identified. The evidence herein solely defines a unique relationship (or link) between the Hepatitis B vaccine and the author’s injury. It identifies the nature of the relationship, the timing of the relationship, and the duration of the relationship. The empirical findings of this study therefore contribute to the material facts surrounding the author’s injury.
Australian regulations state that a medical product must be proved safe, but it does not have to be proved effective. In the author’s case, the HBV received failed on both counts, as it has been demonstrated herein that this vaccine was both unsafe and ineffective! Since vaccines are immunogenic conditioners and manipulators of the genetic environment of their hosts, once a host’s immune system is genetically shifted to a new program, even a self-destructive program, the potential for those artificial changes to remain permanent are significant. Effective immunisation however, from such immune shifts is remote. Finding and replicating the immunogenic key that deactivates or switches off the new programming, without the repressive effects of suppression drugs, is a technology that lies decades away, if it is achievable at all.
Given that the expected immune markers for vaccine causation were fully supported by the empirical data and clinical observations, the proposition at the beginning of this investigation that a foreign immune agent (the vaccine) was entirely responsible for the author’s injury, is fully endorsed. The profile of this harmful relationship is identified as follows:
Profile of Vaccine Causal Link:
The clinical and empirical evidence demonstrates an eight-fold causal link between the Hepatitis B Vaccine and the author’s injury:
1): Negative screening results for pathogens and pre-existing conditions in the extensive serology testing, supports an exclusion diagnosis.
2): Two separate reactions characterised by a constellation of adverse symptoms, causing severe and chronic disruption to the author’s health.
3): The eruption of multiple immune inflammatory markers, namely:
Ø 80% increase in total White Blood Cell levels above the norm.
Ø 3.5 year alteration to neutrophil and lymphocyte cell ratios from the norm, and chronically elevated cytotoxic NK and non-MHCR cells.
Ø Enlargement of the liver lobes and lymph glands, with RHS abdominal pain, despite negative screening results for hepatic viremia.
Ø 300% serum increase in ALT Liver enzyme levels above the norm.
Ø Increases in body temperature (fever) for 2 days, then 22 days, at start of each respective reaction.
Ø Sudden onset of low grade leg paralysis, diffuse myalgias and fatigue.
4): The repeated latency of symptoms (of 22 and 21 days) after each inoculation, links each delay with each respective injection.
5): The recurrence of the same symptoms after re-exposure to the same drug (a Positive Rechallenge), with a marked increase in severity of the second adverse reaction.
6): The long phase distribution of immune disruption (as Acute, Intermediate, & Chronic phases), extending well past documented life cycle time-frames of viral and bacterial infections.
7): The post development of immune intolerances via the digestive pathway to oral antibiotics and certain foods, previously well tolerated. Acquired sensitivities and allergies are expressions of immune condition.
8): The correlation of the author’s adverse symptoms with the vaccine manufacturer’s declared side-effects, as published in their vaccine Product Information Leaflet (PIL).
P.T.