
Report Release Date: 13 December 2004
Mercury Primer Summary Scientists have identified a signature metabolic impairment or "biomarker" in autistic children that strongly suggests that these children would be susceptible to the harmful effects of mercury and other toxic chemical exposures (James 2004a).
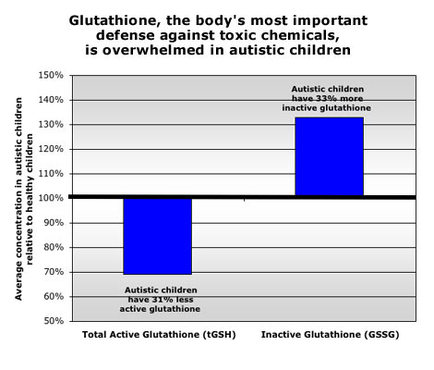
This impairment manifests as a severe imbalance in the ratio of active to inactive glutathione, the body's most important tool for detoxifying and excreting metals. Glutathione works as an antioxidant, keeping in check the potentially destructive process of oxidative stress caused both by normal metabolism and environmental contaminants. Autistic children showed a significant impairment in every one of five measurements of the body's ability to maintain a healthy glutathione defense.
These findings raise serious concerns about children's overall exposure to environmental contaminants. Mercury is of particular concern, however, because of its proven toxicity to the developing brain and nervous system, and documented high exposures from a variety of sources.
One of every six pregnancies is exposed to methyl mercury above EPA's safe level from maternal consumption of contaminated seafood (CDC 2002, Mahaffey 2004). Thimerosal, a preservative in vaccines that is 49 percent ethyl mercury, was a major source of mercury exposure from 1988 through 2002 when it was removed from childhood immunizations at the urging of the Public Health Service and the American Academy of Pediatrics. Elemental mercury from dental amalgams is another potentially important source, but its contribution to overall mercury exposure is less well studied.
The incidence of autism increased 10-fold from 6 in 10,000 in the 1980s (Blaxill 2004), to about 60 in 10,000 today (Autism Alarm, PDF file). These new findings significantly strengthen the possibility that mercury could cause or contribute to autism and other neurodevelopmental disorders by identifying a metabolic imbalance common to nearly all autistic children that would make these children poorly equipped to mount a defense against a number of neurotoxic compounds, including mercury.
These findings could have major implications for public health protections from toxic chemicals in the environment. They identify a subgroup of people at increased risk of harm, and provide important new evidence that policies designed to protect the average person, or even the average child, from chemical exposure, are insufficient to fully protect the public health. Environmental and health officials must evaluate the adequacy of current laws and policies to protect individuals with a heightened sensitivity to chemical exposure.
Finally, these findings raise serious concerns about the studies that have allegedly proven the safety of mercury in vaccines. The epidemiologic studies used to dismiss a causal relationship between autism and thimerosal have assumed that all children have the same resistance to chemical exposure. To properly investigate the potential harm from mercury-containing shots researchers would have to compare autism rates in children with the same type of vulnerability.
Background In 1988, the Centers for Disease Control (CDC) recommended important new additions to the nation's infant immunization program, including three Hepatitis B immunizations (one injected at birth), and three Haemophilis B shots—all delivered by six months of age. Drug companies responded with vaccinations supplied in multiple dose containers preserved with the mercury-based antibacterial thimerosal. Neither the CDC, nor the Food and Drug Administration (FDA), which monitors the safety of vaccinations, expressed concerns at that time about the relatively high doses of mercury that newborn babies and infants would be exposed to through these shots.
A dramatic nationwide increase in autism followed directly on the heels of the abrupt rise in thimerosal exposure (Blaxill 2001). Rates rose from 6 in 10,000 children in the 1980s to 60 in 10,000 today (Blaxill 2004a, American Academy of Pediatrics 2004). In 2003, the Autism Society of America estimated the cost of treating and caring for 1.5 million autistic children at $90 billion per year (Autism Society of America 2003).
To better understand whether or not the dramatic increase in autism was related to the abrupt nationwide increase in exposure to mercury in vaccinations, the CDC conducted its own epidemiologic study, and then convened a panel of the Institute of Medicine (IOM) of the National Academy of Sciences to review the issue independently. On May 17, 2004, the IOM published its final report on the possible link between thimerosal and autism. The IOM rejected "a causal relationship" between the two, and then took the unusual step of recommending the termination of additional research into the subject, stating clearly that, "Further research to find the cause of autism should be directed toward other lines of inquiry" (IOM press release 2004a). Or as put by the chair of the IOM committee, "Available funding for autism research should be channeled to the most promising areas, of which the link with vaccines does not appear to be one" (Barclay 2004). The chief of the national immunization program at the Centers for Disease Control went even further, declaring that only "junk scientists and charlatans" support research into the potential link between thimerosal exposure and autism (Levin 2004).
The IOM's recommendation that research into the potential link between mercury and autism be abandoned is highly unusual coming from an institution built on the notion of free scientific inquiry. Not surprisingly, the statement was cause for concern in some scientific quarters. In spite of these and other concerns, however, the committee's findings remain, on balance, an accurate reflection of the published epidemiologic studies at the time of its release.
What is more important, but largely overlooked, was the committee's own admission that it did not adequately address the leading theory among independent scientists — that autism could be triggered by environmental exposures, including mercury in vaccines, in a subset of vulnerable children. As the IOM panel stated in its final report:
"...the committee cannot rule out, based on the epidemiological evidence, the possibility that vaccines contribute to autism in some small subset or very unusual circumstances" (IOM 2004b).
Or as put by the Chair of the IOM committee, Dr. Marie McCormick, of the Harvard School of Public Health:
"Some children could be particularly vulnerable or susceptible to mercury exposure because of genetic or other differences" (McCormick 2001).
Findings An eighteen-month investigation by Environmental Working Group concludes that scientists have identified a signature metabolic profile or "biomarker" in autistic children that may indeed characterize a "small subset" of susceptible children. These findings represent a potential milestone in our understanding of individual vulnerability to toxic substances, including, but not limited to, mercury. This science turns on its head the IOM's judgment that research into the thimerosal/autism link be abandoned, and instead strengthens significantly the case for additional research in this area. We found that:
Newly published research and follow-up testing by former FDA senior research scientist Dr. Jill James, now of the University of Arkansas for Medical Sciences, has uncovered a unique and consistent metabolic imbalance in autistic children when compared to normal healthy children (James 2004a, 2004b). This impairment manifests as a severe deficit in the body's most important antioxidant and metals detoxifier, glutathione. When compared to normal health children, autistic children showed a significant impairment in every one of five measurements of the body's ability to maintain a healthy glutathione defense. These findings are strong evidence that if these children were exposed to a potentially toxic dose of mercury or other compound they would be much less able to mount an effective defense.
Mercury Primer Summary Scientists have identified a signature metabolic impairment or "biomarker" in autistic children that strongly suggests that these children would be susceptible to the harmful effects of mercury and other toxic chemical exposures (James 2004a).
This impairment manifests as a severe imbalance in the ratio of active to inactive glutathione, the body's most important tool for detoxifying and excreting metals. Glutathione works as an antioxidant, keeping in check the potentially destructive process of oxidative stress caused both by normal metabolism and environmental contaminants. Autistic children showed a significant impairment in every one of five measurements of the body's ability to maintain a healthy glutathione defense.
These findings raise serious concerns about children's overall exposure to environmental contaminants. Mercury is of particular concern, however, because of its proven toxicity to the developing brain and nervous system, and documented high exposures from a variety of sources.
One of every six pregnancies is exposed to methyl mercury above EPA's safe level from maternal consumption of contaminated seafood (CDC 2002, Mahaffey 2004). Thimerosal, a preservative in vaccines that is 49 percent ethyl mercury, was a major source of mercury exposure from 1988 through 2002 when it was removed from childhood immunizations at the urging of the Public Health Service and the American Academy of Pediatrics. Elemental mercury from dental amalgams is another potentially important source, but its contribution to overall mercury exposure is less well studied.
The incidence of autism increased 10-fold from 6 in 10,000 in the 1980s (Blaxill 2004), to about 60 in 10,000 today (Autism Alarm, PDF file). These new findings significantly strengthen the possibility that mercury could cause or contribute to autism and other neurodevelopmental disorders by identifying a metabolic imbalance common to nearly all autistic children that would make these children poorly equipped to mount a defense against a number of neurotoxic compounds, including mercury.
These findings could have major implications for public health protections from toxic chemicals in the environment. They identify a subgroup of people at increased risk of harm, and provide important new evidence that policies designed to protect the average person, or even the average child, from chemical exposure, are insufficient to fully protect the public health. Environmental and health officials must evaluate the adequacy of current laws and policies to protect individuals with a heightened sensitivity to chemical exposure.
Finally, these findings raise serious concerns about the studies that have allegedly proven the safety of mercury in vaccines. The epidemiologic studies used to dismiss a causal relationship between autism and thimerosal have assumed that all children have the same resistance to chemical exposure. To properly investigate the potential harm from mercury-containing shots researchers would have to compare autism rates in children with the same type of vulnerability.
Background In 1988, the Centers for Disease Control (CDC) recommended important new additions to the nation's infant immunization program, including three Hepatitis B immunizations (one injected at birth), and three Haemophilis B shots—all delivered by six months of age. Drug companies responded with vaccinations supplied in multiple dose containers preserved with the mercury-based antibacterial thimerosal. Neither the CDC, nor the Food and Drug Administration (FDA), which monitors the safety of vaccinations, expressed concerns at that time about the relatively high doses of mercury that newborn babies and infants would be exposed to through these shots.
A dramatic nationwide increase in autism followed directly on the heels of the abrupt rise in thimerosal exposure (Blaxill 2001). Rates rose from 6 in 10,000 children in the 1980s to 60 in 10,000 today (Blaxill 2004a, American Academy of Pediatrics 2004). In 2003, the Autism Society of America estimated the cost of treating and caring for 1.5 million autistic children at $90 billion per year (Autism Society of America 2003).
To better understand whether or not the dramatic increase in autism was related to the abrupt nationwide increase in exposure to mercury in vaccinations, the CDC conducted its own epidemiologic study, and then convened a panel of the Institute of Medicine (IOM) of the National Academy of Sciences to review the issue independently. On May 17, 2004, the IOM published its final report on the possible link between thimerosal and autism. The IOM rejected "a causal relationship" between the two, and then took the unusual step of recommending the termination of additional research into the subject, stating clearly that, "Further research to find the cause of autism should be directed toward other lines of inquiry" (IOM press release 2004a). Or as put by the chair of the IOM committee, "Available funding for autism research should be channeled to the most promising areas, of which the link with vaccines does not appear to be one" (Barclay 2004). The chief of the national immunization program at the Centers for Disease Control went even further, declaring that only "junk scientists and charlatans" support research into the potential link between thimerosal exposure and autism (Levin 2004).
The IOM's recommendation that research into the potential link between mercury and autism be abandoned is highly unusual coming from an institution built on the notion of free scientific inquiry. Not surprisingly, the statement was cause for concern in some scientific quarters. In spite of these and other concerns, however, the committee's findings remain, on balance, an accurate reflection of the published epidemiologic studies at the time of its release.
What is more important, but largely overlooked, was the committee's own admission that it did not adequately address the leading theory among independent scientists — that autism could be triggered by environmental exposures, including mercury in vaccines, in a subset of vulnerable children. As the IOM panel stated in its final report:
"...the committee cannot rule out, based on the epidemiological evidence, the possibility that vaccines contribute to autism in some small subset or very unusual circumstances" (IOM 2004b).
Or as put by the Chair of the IOM committee, Dr. Marie McCormick, of the Harvard School of Public Health:
"Some children could be particularly vulnerable or susceptible to mercury exposure because of genetic or other differences" (McCormick 2001).
Findings An eighteen-month investigation by Environmental Working Group concludes that scientists have identified a signature metabolic profile or "biomarker" in autistic children that may indeed characterize a "small subset" of susceptible children. These findings represent a potential milestone in our understanding of individual vulnerability to toxic substances, including, but not limited to, mercury. This science turns on its head the IOM's judgment that research into the thimerosal/autism link be abandoned, and instead strengthens significantly the case for additional research in this area. We found that:
Newly published research and follow-up testing by former FDA senior research scientist Dr. Jill James, now of the University of Arkansas for Medical Sciences, has uncovered a unique and consistent metabolic imbalance in autistic children when compared to normal healthy children (James 2004a, 2004b). This impairment manifests as a severe deficit in the body's most important antioxidant and metals detoxifier, glutathione. When compared to normal health children, autistic children showed a significant impairment in every one of five measurements of the body's ability to maintain a healthy glutathione defense. These findings are strong evidence that if these children were exposed to a potentially toxic dose of mercury or other compound they would be much less able to mount an effective defense.
Source: James 2004b
The finding of a significant glutathione deficit in autistic children provides a biological basis for integrating many facets of autism that have baffled researchers attempting to pin the autism epidemic on a single gene or chemical exposure. The implications of these findings extend well beyond thimerosal and autism. Reduced antioxidant defense may characterize a group of individuals who are demonstrably more sensitive to the effects of a range of toxic chemical exposures, and shed light on increasing rates of related learning and behavioral disorders. These findings raise serious concerns about the studies that have allegedly proven the safety of mercury in vaccines. While Dr. James' results do not prove that mercury causes autism, they significantly strengthen this possibility. The epidemiologic studies used to dismiss a causal relationship between mercury and autism assumed that all children have the same resistance to chemical exposure. Given James' finding that autistic children would be much more sensitive to certain chemical contaminants, studies that do not acknowledge these vulnerabilities cannot be used to dismiss the relationship between environmental chemicals, including mercury, and the disease. When James' results are considered together with the existing body of science, including other recently published research, the weight of the evidence now strongly supports increased research into the relationship between thimerosal and autism as well as other neurodevelopmental and neurodegenerative disorders.
Recommendations
Research
The findings by James significantly strengthen the science supporting a connection between mercury and autism. Contrary to the recommendation of the Institute of Medicine, that research on the relationship between mercury and autism essentially be abandoned, the weight of the evidence in the basic biological sciences now supports accelerated funding and research into the biological pathways and genetic mechanisms that may make some individuals more vulnerable to mercury and a host of other environmental toxins. We recommend increased federal support for research in this area.
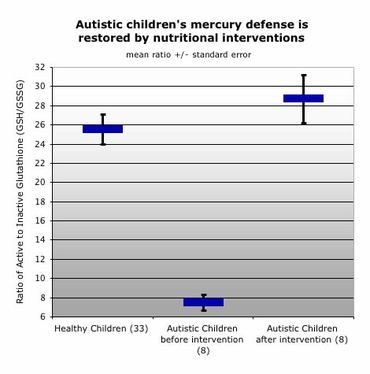
A small follow-up group of children in this study have benefited markedly when their impaired antioxidant defense was restored. This provides important clues about treatments that could derive from increased funding for research in this area.
The finding of a significant glutathione deficit in autistic children provides a biological basis for integrating many facets of autism that have baffled researchers attempting to pin the autism epidemic on a single gene or chemical exposure. The implications of these findings extend well beyond thimerosal and autism. Reduced antioxidant defense may characterize a group of individuals who are demonstrably more sensitive to the effects of a range of toxic chemical exposures, and shed light on increasing rates of related learning and behavioral disorders. These findings raise serious concerns about the studies that have allegedly proven the safety of mercury in vaccines. While Dr. James' results do not prove that mercury causes autism, they significantly strengthen this possibility. The epidemiologic studies used to dismiss a causal relationship between mercury and autism assumed that all children have the same resistance to chemical exposure. Given James' finding that autistic children would be much more sensitive to certain chemical contaminants, studies that do not acknowledge these vulnerabilities cannot be used to dismiss the relationship between environmental chemicals, including mercury, and the disease. When James' results are considered together with the existing body of science, including other recently published research, the weight of the evidence now strongly supports increased research into the relationship between thimerosal and autism as well as other neurodevelopmental and neurodegenerative disorders.
Recommendations
Research
The findings by James significantly strengthen the science supporting a connection between mercury and autism. Contrary to the recommendation of the Institute of Medicine, that research on the relationship between mercury and autism essentially be abandoned, the weight of the evidence in the basic biological sciences now supports accelerated funding and research into the biological pathways and genetic mechanisms that may make some individuals more vulnerable to mercury and a host of other environmental toxins. We recommend increased federal support for research in this area.
A small follow-up group of children in this study have benefited markedly when their impaired antioxidant defense was restored. This provides important clues about treatments that could derive from increased funding for research in this area.
Several studies are underway to explore the relationship between thimerosal-containing vaccines and autism in greater detail—including a follow-up study underway by the CDC (Verstraeten 2004). The power of these studies would be dramatically enhanced if they included Dr. James' simple blood test to examine the antioxidant capacity of autistic and healthy children as a factor that modifies an individual's sensitivity to mercury toxicity.
Policy Reform: Environmental Health
James' findings also have major implications for public health protections and pollution control. They potentially identify a subgroup of people with dramatically increased risk of harm from industrial chemicals, and provide important new evidence that policies designed to protect the average person, or even the average child, from chemical exposure, are insufficient to fully protect the public health. Children with the metabolic profile James has identified may be more susceptible to a vast number of common pollutants, from arsenic in drinking water and pressure-treated wood, to air pollution from cars and power plants. Environmental and health officials must evaluate the adequacy of current laws and policies to protect individuals with a heightened sensitivity to chemicals exposure.
Policy Reform: Immunizations
The Environmental Working Group strongly supports the standard battery of childhood immunizations recommended by the American Academy of Pediatrics and the CDC. Clearly, vaccinations have led to many major advances in public health. At the same time, EWG recommends the removal of thimerosal and all mercury-based preservatives from all vaccines in the United States, as is currently required by law in California and Iowa.
As individual states and many industrialized countries have phased out or banned the use of the mercury-based preservative in vaccines, the use of immunizations preserved with thimerosal continues unabated in the developing world. Precisely because of the clear public health benefits of vaccinations, the limited access to refrigeration, and the need to deliver vaccines in multiple dose containers in these countries, we urge the World Health Organization and multinational drug companies to move quickly to develop and adopt an alternative, low cost, effective preservative that is safer than mercury-based thimerosal.
Mercury Primer
Mercury, a potent toxic metal that targets the developing brain and nervous system, is challenging lead as the number one environmental health threat to American children. According to the EPA's top mercury scientist, one out of every six children born in the United States is exposed to levels of methyl mercury during pregnancy that exceed what the Agency considers safe (Mahaffey 2004). The principal source of high fetal methyl mercury exposure is maternal consumption of contaminated seafood, primarily canned tuna. Pregnant women who eat significant quantities of large ocean-going fish could expose their babies to amounts of mercury that are well above the government's recommended safe levels.
In March, 2004, the Food and Drug Administration revised their mercury seafood advisory to include a specific warning about consumption of canned albacore tuna. Pregnant women and children are advised to eat no more than one six ounce can of albacore tuna per week. The advisory, however, provides no consumption advice for a number of fish where high mercury levels are a concern, including tuna steaks, sea bass, halibut, and many others. The Environmental Working Group has filed a legal challenge to the FDA mercury seafood advisory, charging that it is not based on the best available science on seafood contamination and mercury risk levels to the developing fetus.
But contaminated seafood is not the only source of mercury exposure for the developing fetus or infant. Mercury amalgam dental fillings are a potentially significant source of fetal mercury exposure, although precise amounts are not well characterized. And from 1988 through about 2002, children were exposed to significant doses of mercury from birth through six months of age in the form of a mercury-based preservative, thimerosal, used in routine childhood immunizations. Children born to Rh negative mothers were also exposed to mercury in-utero when their mothers received a mercury-containing RhoGAM shot. The flu shot is another source of fetal and infant mercury exposure. The health impact of mercury exposure through vaccinations has been the source of intense debate because of significant changes in the vaccination regimen from 1988 through 1991 that increased neonatal and infant exposure to mercury.
In 1988, the Centers for Disease Control (CDC) recommended important new additions to the nation's infant immunization program, including three Hepatitis B immunizations (one injected at birth), and three Haemophilis B shots—all delivered by six months of age. Drug companies responded with vaccinations supplied in multiple dose containers preserved with the mercury-based antibacterial thimerosal. Neither the CDC, nor the Food and Drug Administration (FDA), which monitors the safety of vaccinations, expressed concerns at that time about the relatively high doses of mercury that newborn babies and infants would be exposed to through these shots.
Drug companies were similarly silent on the matter, although internal company documents show that they were aware of the potent neurotoxic effects of mercury as early as the 1940s. Notably, the FDA banned the sale of topically applied thimerosal antibiotics in the 1980s due to severe, even crippling, adverse skin reactions in sensitive individuals.
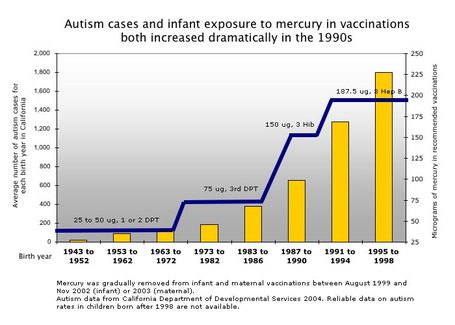
The amount of mercury in the standard battery of childhood immunizations more than doubled between 1988 and 1991 when these additional shots were added to the early childhood vaccination regimen. Throughout the 1990s, children received nine mercury-containing vaccinations within their first six months of life, including the unprecedented injection of a mercury-containing vaccine at birth, and up to three shots given in a single day at 2-, 4-, and 6-months. The average two-month old baby vaccinated with thimerosal-containing shots in the 1990s received a single day dose of mercury that was between 100 and 125 times the government's long-term safe exposure level.
Drug companies used thimerosal as a vaccine preservative to allow multiple injections to be shipped and stored in single containers. Thimerosal is 49 percent ethyl mercury, a widely recognized and potent neurotoxin. After more than a decade of nationwide, high childhood exposures, it was removed from childhood vaccinations between 1999 and 2002, at the urging of the Public Health Service and the American Academy of Pediatrics, but is still present in most flu vaccines. California and Iowa have banned mercury-containing thimerosal from all vaccinations, and Missouri and Nebraska have legislation in progress.
Part 1:
Environmental triggers are a neglected component of autism research There is no doubt that an environmental factor has contributed to the dramatic increase in the incidence of autism over the past 15 years. Genetic factors are a component in the condition—concurrent rates of autism in identical twins approach 90 percent—but rates of inherited genetic diseases do not change abruptly in one generation, whereas autism rates skyrocketed during the 1990s. Rates of autism in the United States increased from fewer than 6 cases per 10,000 children in the 1980s to more than 60 per 10,000 children today (Blaxill 2004a). The American Academy of Pediatrics and the Centers for Disease Control (CDC) currently estimate that autism affects one in every 166 children (AAP 2004). Improved diagnosis does not adequately account for this increase (Blaxill 2004a, Croen 2003).
Autism is a complex neurological disorder characterized by severely impaired social interaction and language skills. The social and economic costs of the autism epidemic are staggering. In 2003, the Autism Society of America estimated the cost of treating the 1.5 million cases of autism to be $90 billion per year rising to $200-400 billion by 2010 (ASA 2003). In addition to the economic costs of treatment, autism is a tremendous burden to family members who must provide lifelong care to loved ones affected by the disorder.
There has been little progress in identifying pre- and post-natal environmental exposures that might trigger the severe impacts to brain development, intestinal and immune dysregulation that characterize autism disorders (London 2000). Hundreds of studies have explored the genetic roots of the autism epidemic, but none has uncovered a single gene or vulnerability to account for more than a fraction of cases.
Children's exposure to mercury in immunizations has been a long-standing concern of autism advocates—and for good reason. Mercury is highly toxic to brain cells and other body systems impacted by autism. Several classic features of autism—speech loss and loss of social and communication skills—are signature traits of mercury poisoning. Many parents report children slipping into autism shortly after receiving multiple mercury-containing vaccinations.
One in every six children born in the United States, or 630,000 per year, are exposed to potentially unsafe levels of mercury during pregnancy from contaminated seafood in the maternal diet, creating a background level of exposure that could be exacerbated by cumulative and frequent mercury doses from vaccinations (Mahaffey 2004). Virtually all children in the U.S. were vaccinated repeatedly with mercury-containing vaccine during the 1990s; if a percentage of these children had a metabolic imbalance that increased their vulnerability to mercury, this near universal exposure could help explain the dramatic nationwide increase in autism that followed directly on the heels of this abrupt rise in thimerosal use. The findings discussed here, that autistic children share a common deficit in antioxidant protection, call into question the conclusion that mercury in vaccines is uniformly safe for all children, and underscores the need for a broader look at the role of environmental chemicals in the autism epidemic.
Every existing study that has failed to find a link between thimerosal exposure and autism has looked at disease rates in vaccinated children without regard to their individual metabolism. To properly investigate the role of mercury-containing shots in a vulnerable group, researchers would have to compare autism rates in children with the same type of vulnerability. This has not been done.
Important New Finding offers clues to autism prevention and treatment In an exciting breakthrough, Dr. Jill James of the University of Arkansas School of Medicine has documented a unique metabolic profile in 95 autistic children with regressive autism. (James 2004a, 2004b) Regressive autism is a form of the disease in which children develop normally for a certain period before losing previously acquired language or behaviors and being diagnosed with autism.
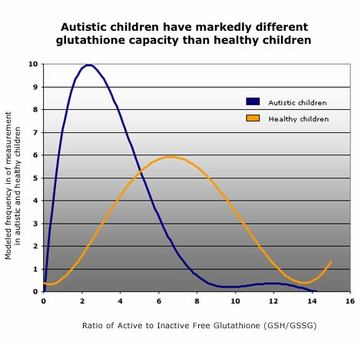
The metabolic profile in the James study children manifests as a severe imbalance in the ratio of active to inactive glutathione in autistic children, compared to a group of healthy control children (James 2004a, 2004b). Glutathione, a potent antioxidant, is the body's most important tool for detoxifying and excreting metals.
The amount of mercury in the standard battery of childhood immunizations more than doubled between 1988 and 1991 when these additional shots were added to the early childhood vaccination regimen. Throughout the 1990s, children received nine mercury-containing vaccinations within their first six months of life, including the unprecedented injection of a mercury-containing vaccine at birth, and up to three shots given in a single day at 2-, 4-, and 6-months. The average two-month old baby vaccinated with thimerosal-containing shots in the 1990s received a single day dose of mercury that was between 100 and 125 times the government's long-term safe exposure level.
Drug companies used thimerosal as a vaccine preservative to allow multiple injections to be shipped and stored in single containers. Thimerosal is 49 percent ethyl mercury, a widely recognized and potent neurotoxin. After more than a decade of nationwide, high childhood exposures, it was removed from childhood vaccinations between 1999 and 2002, at the urging of the Public Health Service and the American Academy of Pediatrics, but is still present in most flu vaccines. California and Iowa have banned mercury-containing thimerosal from all vaccinations, and Missouri and Nebraska have legislation in progress.
Part 1:
Environmental triggers are a neglected component of autism research There is no doubt that an environmental factor has contributed to the dramatic increase in the incidence of autism over the past 15 years. Genetic factors are a component in the condition—concurrent rates of autism in identical twins approach 90 percent—but rates of inherited genetic diseases do not change abruptly in one generation, whereas autism rates skyrocketed during the 1990s. Rates of autism in the United States increased from fewer than 6 cases per 10,000 children in the 1980s to more than 60 per 10,000 children today (Blaxill 2004a). The American Academy of Pediatrics and the Centers for Disease Control (CDC) currently estimate that autism affects one in every 166 children (AAP 2004). Improved diagnosis does not adequately account for this increase (Blaxill 2004a, Croen 2003).
Autism is a complex neurological disorder characterized by severely impaired social interaction and language skills. The social and economic costs of the autism epidemic are staggering. In 2003, the Autism Society of America estimated the cost of treating the 1.5 million cases of autism to be $90 billion per year rising to $200-400 billion by 2010 (ASA 2003). In addition to the economic costs of treatment, autism is a tremendous burden to family members who must provide lifelong care to loved ones affected by the disorder.
There has been little progress in identifying pre- and post-natal environmental exposures that might trigger the severe impacts to brain development, intestinal and immune dysregulation that characterize autism disorders (London 2000). Hundreds of studies have explored the genetic roots of the autism epidemic, but none has uncovered a single gene or vulnerability to account for more than a fraction of cases.
Children's exposure to mercury in immunizations has been a long-standing concern of autism advocates—and for good reason. Mercury is highly toxic to brain cells and other body systems impacted by autism. Several classic features of autism—speech loss and loss of social and communication skills—are signature traits of mercury poisoning. Many parents report children slipping into autism shortly after receiving multiple mercury-containing vaccinations.
One in every six children born in the United States, or 630,000 per year, are exposed to potentially unsafe levels of mercury during pregnancy from contaminated seafood in the maternal diet, creating a background level of exposure that could be exacerbated by cumulative and frequent mercury doses from vaccinations (Mahaffey 2004). Virtually all children in the U.S. were vaccinated repeatedly with mercury-containing vaccine during the 1990s; if a percentage of these children had a metabolic imbalance that increased their vulnerability to mercury, this near universal exposure could help explain the dramatic nationwide increase in autism that followed directly on the heels of this abrupt rise in thimerosal use. The findings discussed here, that autistic children share a common deficit in antioxidant protection, call into question the conclusion that mercury in vaccines is uniformly safe for all children, and underscores the need for a broader look at the role of environmental chemicals in the autism epidemic.
Every existing study that has failed to find a link between thimerosal exposure and autism has looked at disease rates in vaccinated children without regard to their individual metabolism. To properly investigate the role of mercury-containing shots in a vulnerable group, researchers would have to compare autism rates in children with the same type of vulnerability. This has not been done.
Important New Finding offers clues to autism prevention and treatment In an exciting breakthrough, Dr. Jill James of the University of Arkansas School of Medicine has documented a unique metabolic profile in 95 autistic children with regressive autism. (James 2004a, 2004b) Regressive autism is a form of the disease in which children develop normally for a certain period before losing previously acquired language or behaviors and being diagnosed with autism.
The metabolic profile in the James study children manifests as a severe imbalance in the ratio of active to inactive glutathione in autistic children, compared to a group of healthy control children (James 2004a, 2004b). Glutathione, a potent antioxidant, is the body's most important tool for detoxifying and excreting metals.
Metabolite Number of Healthy Controls Average in Autistic Children Average in Healthy Children Difference in autistic group p-value Homocysteine (umol/L) 75 5.5 5.9 7% less 0.05 Cysteine (umol/L) 75 161 205 22% less <0.0001 Active Glutathione: Total:tGSH
(umol/L) 75 5.1 7.5 31% less <0.0001 Free:
fGSH (umol/L) 49 1.5 2.1 30% less <0.0001 Inactive Glutathione: GSSG (nmol/L) 49 0.41 0.31 34% more 0.0015 Glutathione ratio (unitless) tGSH/GSSG 49 16.7 27.6 40% less <0.0001 fGSH/GSSG 49 5.0 7.1 30% less <0.0001
(umol/L) 75 5.1 7.5 31% less <0.0001 Free:
fGSH (umol/L) 49 1.5 2.1 30% less <0.0001 Inactive Glutathione: GSSG (nmol/L) 49 0.41 0.31 34% more 0.0015 Glutathione ratio (unitless) tGSH/GSSG 49 16.7 27.6 40% less <0.0001 fGSH/GSSG 49 5.0 7.1 30% less <0.0001
Source: James 2004b
The James study shows that children with regressive autism have consistently elevated levels of oxidative stress as compared to normal healthy children. Individuals with reduced glutathione antioxidant capacity will be under chronic oxidative stress and will be more vulnerable to toxic compounds that act primarily through oxidative damage, including mercury (James 2004). Oxidative stress plays a key role in several important degenerative diseases of the brain and nervous system, including Alzheimer's, Parkinson's, Huntington's disease, and schizophrenia (Shulz 2000, Granot 2004).
The James study shows that children with regressive autism have consistently elevated levels of oxidative stress as compared to normal healthy children. Individuals with reduced glutathione antioxidant capacity will be under chronic oxidative stress and will be more vulnerable to toxic compounds that act primarily through oxidative damage, including mercury (James 2004). Oxidative stress plays a key role in several important degenerative diseases of the brain and nervous system, including Alzheimer's, Parkinson's, Huntington's disease, and schizophrenia (Shulz 2000, Granot 2004).
Dr. James' findings shift the focus of research from single genes to a broader metabolic disorder shared by the vast majority of autistic children. They also indicate a mechanism by which autistic children would be more sensitive to chemicals that cause oxidative stress and damage their developing brain and nervous system. In another recent study Dr. James found that glutathione protects brain cells from oxidative damage and cell death caused by thimerosal exposure (James 2005). Numerous studies have confirmed the toxicity of metals to brain cells at doses similar to those experienced by vaccinated children (Makani 2002, Shanker 2003, Baskin 2003, Waly 2004, Ueha-Ishibashi 2004).
These findings raise serious concerns about the studies that have allegedly proven the safety of mercury in vaccines. While Dr. James' results do not prove that mercury in vaccinations causes autism or other neurodevelopmental disorders, they significantly strengthen that possibility by identifying a metabolic imbalance common to nearly all autistic children that would make these children poorly equipped to mount a defense against the large doses of mercury they all received via vaccines.
Oxygen radicals damage the brain and nervous system Autistic children's inability to combat oxidative stress can lead to many health problems. Oxidative stress is caused by oxygen radicals — highly unstable chemicals that react with and destroy healthy cells. These free oxygen radicals are produced by the body in manageable amounts as byproducts of normal body metabolism, but their prevalence can be exacerbated by exposure to environmental chemicals. Oxygen radicals damage cells by reacting with proteins, DNA, carbohydrates, and fats, setting off chain reactions that can only be stopped by a cell's antioxidant defense system. In the process they disrupt cell functions and interfere with signals sent between cells in the body, which can lead to auto-immunity (Klein 2003).
Oxidative damage is counteracted by the body's antioxidant systems, which convert oxygen radicals into harmless byproducts. Oxidative stress occurs when oxygen radicals overwhelm the capacity of the body's antioxidant systems. Oxidative stress affects many body systems. It damages cell membrane structure (lipids), the cell machinery that performs the essential work of the cells (proteins), and the body's ability to regulate cell growth and protein synthesis (DNA and RNA). Oxidative stress is associated with premature aging of cells, and can lead to tissue inflammation, damaged cell membranes, autoimmunity and cell death (Klein 2003). Glutathione is the most important antioxidant for metals detoxification and excretion.
The brain and nervous system are particularly vulnerable to oxidative stress due to limited antioxidant capacity. The brain makes up about two percent of a person's mass but consumes 20 percent of their metabolic oxygen. The vast majority of this energy is used by the neurons (Shulman 2004). Some brain cells, like neurons, cannot make glutathione, but instead rely on surrounding astrocyte cells to provide useable glutathione precursors. Because the brain has limited access to the bulk of antioxidants produced by the body, neurons are the first cells to be affected by a shortage of antioxidants, and are most susceptible to oxidative stress. Researchers studying antioxidant protection of neurons are finding short windows during development of high vulnerability to oxidative stress (Perry 2004).
Children are more vulnerable than adults to oxidative stress due to their naturally low glutathione levels from conception through infancy (Erden-Inal 2003, Ono 2001). Risks created by this natural deficit in detoxification capacity in infants are compounded by the fact that mercury and other environmental chemicals that invoke oxidative stress are found at higher concentrations in the developing infant than in their mothers and appear to accumulate in the placenta.
In addition to this natural variability in antioxidant status with age, a person's genes play a strong role in their ability to make antioxidants in response to oxidative stress. A host of genes determine the speed and responsiveness of antioxidant production and recycling. Some genes common in one quarter to one half of the U.S. population reduce glutathione activity and are linked with increased odds of several cancers (Hallier 1994, Engel 2002). People with gene deletions for two types of glutathione genes (GST M1 and T1) are more likely to have allergic reactions to the mercury-based preservative thimerosal (Westphal 2000).
Environmental chemicals that provoke oxidative stress could contribute to autism or other health problems During a typical day children and pregnant women are exposed to many different types of environmental chemicals that cause oxidative stress. These exposures add up, creating special concerns for infants and small children due to age-related sensitivity that derives from naturally low glutathione levels. This natural age-related vulnerability is exacerbated in individuals with impaired glutathione ratios. If these children were exposed to a high dose of any compound that produced significant oxidative stress, they would be less able to detoxify and excrete the compound.
Pervasive environmental contaminants like air pollutants from power plants and auto exhaust, pesticides, heavy metals and food additives all produce some degree of oxidative stress. Fine particulate matter and diesel exhaust both provoke tremendous oxidative stress and deplete glutathione (Li 2002). Oxygen radicals wreak havoc in the lungs of asthmatic children. The pain reliever acetaminophen and alcohol both provoke oxidative stress, but their combined effects are much more potent than either chemical alone.
Exposure to the pesticides maneb and paraquat can push neuron cells already under oxidative stress over a threshold of toxicity and "act as an additional insult to the system and prevent the normal recovery of [antioxidant] defenses" (Barlow 2005). Researchers have concluded that maneb disruptions to cells might cause neurodegeneration "especially with concurrent exposures to other environmentally relevant oxidative stressors, such as paraquat" (Barlow 2005). When they dosed pregnant mice with these pesticides the male offspring showed permanent alterations to neurological systems and enhanced susceptibility as an adult to paraquat (Barlow 2004).
PCBs induce a concentration-dependent increase in oxygen radicals. Cells with low levels of available glutathione are more sensitive to PCBs while cells pre-treated with antioxidants had reduced radical production and less cell death (Lee 2004).
Heavy metals—mercury, cadmium, chromium, cobalt, lead, antimony, nickel and others—are a major source of oxidative stress that are commonly detected in air, soil, water and food. Arsenic and chromium in pressure-treated wood, mercury in fish and vaccines, lead in paint, and metals in soil or drinking water are chronic if not daily sources of oxidative stress in the child's environment.
Glutathione is one of the bodys most important mechanism of heavy metal detoxification and excretion. Some metals—copper, chromium, iron and vanadium—directly provoke oxygen radical formation. Glutathione binds with these compounds as well as other metals—cadmium, lead, mercury, and nickel (Stohs 1995). The resulting, water-soluble chemical is more easily filtered out of the body. People with less 'active glutathione' will not be able to excrete metals as quickly. For example, cells treated with chemicals to inhibit glutathione recycling are much more sensitive to manganese toxicity (Desole 1997). People chronically exposed to arsenic in drinking water have increased oxidative damage and decreased antioxidant potential (Wu 2001).
Numerous studies link thimerosal with oxidative stress to the brain and neurological system at concentrations similar to those that were experienced by children vaccinated in the 1990s. Researchers measured mercury concentrations between 10 and 30 nanomoles per liter (nM) in premature infants given a single Hepatitis B shot at birth (Stajich 2000). Mercury concentrations ranging from 4 to 21 nM are reported in young children when measurements were collected 3 to 20 days after vaccination (Pichichero 2002). Four recent studies of thimerosal toxicity to human brain cells report oxidative damage, interruption of methylation, and decreased cell energy resulting from thimerosal exposure in the range of exposure overlapping with those for vaccinated children in the 1990s (Waly 2004, Baskin 2003, Ueha-Ishibashi 2004, Makani 2002). Several studies documented the protective benefits of antioxidants, especially glutathione, which attenuate the damages caused by thimerosal (Makani 2004, James 2005, Shanker 2003).
Impaired antioxidant production provides a common rationale for many disparate features of autistic disorders The identification of reduced antioxidant capacity as a common impairment in autistic children is an important breakthrough that should guide research into the autism epidemic. It strongly suggests that glutathione is a factor that mediates the relationship between environmental chemicals and autism, and for the first time provides a plausible biological link between several trademark features of the disorder that have baffled researchers searching for a single gene or chemical exposure that is triggering autism.
For example, scientists have failed to explain why autism rates are much higher in males, why autism manifests in some children after a period of healthy development, and why autistic children develop intestinal and autoimmune disorders at high rates. Antioxidant imbalance, particularly glutathione deficit, may be the unifying factor that links these apparently disparate symptoms and provides a clue to interventions that could treat autism. Each of these seemingly disconnected features of autism are strongly associated with glutathione capacity.
Autism rates higher, Glutathione levels lower in males
Males make up 70 percent of all autism cases, as well as the majority of children diagnosed with learning disabilities and attention deficit disorder. New research attributes weaker antioxidant capacity in young males with greater vulnerability in their brain and nervous systems, potentially effecting vulnerability to mercury and autism. Women and girls, in contrast, have lower levels of inactive antioxidant chemicals (Rush 2003). Estrogen is a powerful antioxidant that confers substantial benefits against free-radical mediated damage in aging. Male rats have four times higher rate of oxidative damage to mitochondrial DNA, which the authors pose as a reason for female's longer lifespan in many species including humans (Borrás 2003).
The difference in antioxidant capacity between males and females is most pronounced in newborns. Studies using tissue samples from newborn infants reveal significantly higher glutathione levels, glutathione production, and cell survival in response to oxidative stress in cells from girls compared to boys (Lavoie 1997). Studies of brain injury in newborns have found that inherently stronger glutathione capacity in females protects their brain cells from damage after a traumatic injury. Glutathione concentrations remain constant in females but they drop by as much as 80 percent in males after a brain injury (Du 2004). Similar studies found increased brain damage to children younger than four years old when their antioxidant systems are immature and glutathione levels are lower (Fan 2003).
Glutathione deficit may be responsible for intestinal disorders in autistic children
The reduced concentrations of glutathione Dr. James measured in study children may explain common intestinal ailments noted in autistic children. Glutathione is vital to proper functioning of the intestines. Deficits in glutathione cause degeneration of the jejunum and colon (Martensson 1990). Research suggests that oral administration of glutathione protects intestines against toxicity associated with inflammatory diseases, oxidative damage, and other toxins (Martensson 1990). Rodent studies highlight the role of glutathione in preventing positively charged substances—like metals—from passing through the gut (Samiec 2000). Laboratory studies have also demonstrated that treatment with glutathione precursors can protect the gut from different types of free-radical-mediated injury (Jefferies 2003).
Autistic children commonly suffer from intestinal disorders. In these 'leaky gut' disorders undigested proteins pass through the gut and cause oxidative damage to the brain and nervous system (White 2003). This is similar to PKU, a metabolic disorder in which the toxic accumulation of undigested phenylalanine causes oxidative damage leading to autistic-like symptoms. PKU can be averted in laboratory animals by antioxidant supplementation (Martinez-Cruz 2002). Many parents find that their autistic children's behavior and cognition improve when they eliminate milk and wheat from their diets, indicating that their inflamed intestines my be allowing the passage of undigested proteins that exacerbate their oxidative stress.
Glutathione's role in autism and auto-immunity
Autoimmune diseases are conditions in which the immune system targets the body itself instead of bacteria or other foreign objects. Autoimmunity can be triggered when genetically susceptible people are exposed to an environmental chemical or virus. Oxidative stress also plays an important role in autoimmunity by disrupting cell signaling. T lymphocytes are made less active or hypo-responsive when they are exposed to oxygen radicals. T lymphocytes regain normal responsiveness when the antioxidants N-acetyl cysteine (Cemerski 2002) and other glutathione precursors are added to the system (Hehner 2000).
A recent investigation reported chronic inflammation in the brains of autistic patients, resulting from an over-active immune system, a sign of autoimmunity (Vargas 2004). The inflammation indicates that the brain is responding to a process that is stressing or damaging brain cells, a process which might include oxygen radicals.
The weight of the evidence supports a fresh look at the mercury-autism hypothesis Both autism and mercury exposure are characterized by functional impairment to speech, language and behavior (Bernard 2001, Blaxill 2004b). Recent studies also suggest that the same key regions of the brain are affected in both cases (Limke 2004, Kates 2004). At the same time, episodes of severe mercury exposure reveal that there is no single manifestation of mercury poisoning. In fact, children exposed to high levels of mercury during gestation and infancy have suffered from strikingly different diseases.
Minamata disease resulted from in-utero exposure to mercury-contaminated fish. Children with Minamata disease had symptoms indistinguishable from mental retardation or cerebral palsy (Kondo 2000). Acrodynia resulted from mercury in infant teething powders in the early 1900s. Children with Acrodynia suffered peeling and reddened skin on their hands and feet, and heightened sensitivity to light (Warkany 1966).
Individual susceptibility played an important role in both disorders. Although thousands of children were treated with mercury-containing teething powders, only one in 500 to one in 1,000 children who were exposed developed Acrodynia (Warkany 1966). The role of individual sensitivity made it extremely difficult to link mercury exposure with what was, at the time, a new and bizarre disease. Similarly, when children have been exposed to high levels of mercury in foods, only a small group develop severe mercury poisoning while thousands are apparently unharmed (Jalili 1961, Kondo 2000).
Dr. James' findings clearly reveal a mechanism by which autistic children would be predisposed to mercury-related oxidative damage to their developing brain and nervous system. Several additional pieces of evidence strengthen the potential link between mercury exposure and autism in children with abnormal antioxidant capacity. These include:
The indisputable toxicity of mercury to the brain, particularly the developing brain (Limke 2004, Clarkson 2002, Mahaffey 1999). Peer-reviewed reports showing that autistic children are extremely poor at ridding their bodies of mercury as measured by mercury hair levels (Holmes 2003). The recent finding that autism-like symptoms are triggered by thimerosal in mice with a predisposition to autoimmunity (Hornig 2004). The fact that the prevalence of autism in boys is four times that in girls, and that boys have elevated incidence of damage from mercury exposure in epidemiologic studies (Vahter 2002). Mercury targets brain cells
Pre-natal and early life mercury exposures cause multiple impacts to basic brain development by disrupting the division and migration of neuronal cells (Mahaffey 1999). Mercury creates oxidative stress that directly kills brain cells. Human beings accumulate more mercury in the brain than in blood or other organs. Organic mercury actively transported through the blood—brain barrier accumulates in the highest concentrations in the cerebellum, especially the neuronal cells (Limke 2004). The cerebellum is the brain region associated with movement and cognition, and a key region targeted by toxic chemicals (Fonnum 2000), and a region of impairment in autistic patients (McAlonan 2004).
Dr. James investigated the effect of thimerosal on human brain astrocyte and neuron cells. She found that astrocytes have higher levels of glutathione compared to neurons and were more resistant to the cytotoxic effects of thimerosal (James 2005). Mercury was less toxic to human brain cells pretreated with glutathione or a glutathione precursor N-acetyl cysteine, which is used as a treatment for mercury intoxication and it is thought to speed mercury excretion from the body (Ballatori 1998). Similar studies have documented oxidative damages of mercury and glutathione protection to T cells, astrocytes, neurons and fibroblasts (Makani 2002, Shanker 2003).
Immune symptoms
In the summer of 2004, researchers at Columbia's Mailman School of Public Health reported symptoms similar to autism in thimerosal-exposed mice. Thimerosal was administered to three strains of laboratory mice at exposures that replicated infant exposure in the 1990s. Only the mouse strain with a predisposition to autoimmunity was affected by thimerosal exposure. These mice had significant growth delay, reduced locomotion, exaggerated response to novelty, and changes in the brain and nervous system that were suggestive of autism (Hornig 2004).
Metal metabolism and regression
Unlike most substances that are toxic to the brain, there is a significant lag time between exposure to either mercury or thimerosal, and the emergence of the symptoms of mercury poisoning. The length of the lag period depends on the severity of exposures. The delay between first exposure and on-set of symptoms of mercury poisoning has been attributed to the gradual depletion of the brain's compensatory responses, chiefly glutathione and other antioxidants (Weiss 2002).
Autism often is diagnosed after a period of seemingly healthy development. Regressive children lose previously acquired skills such as speech and mobility, or fail to progress in their development. The role that oxidative stress and environmental chemicals play in regressive autism is unknown, but studies finding reduced metal excretion in autistic children point to different dynamics in regressive autism.
A recent publication by physician Amy Holmes reported that autistic children had significantly lower levels of mercury in their hair relative to non-autistic children, suggesting greater accumulation of mercury in the body due to reduced excretion capabilities (Holmes 2003). Hair samples were analyzed from 94 autistic children and 45 non-autistic children between one and two years of age and the autistic children had significantly lower levels of mercury in their hair samples (0.47 vs. 3.63 ppm).
For non-autistic children the level of mercury in the hair sample was strongly correlated with the mother's exposure to mercury in dental fillings, fish consumption and mercury-containing RhoGAM vaccinations during pregnancy. In autistic children there was no correlation, hair levels were always low, even in cases where elevated maternal mercury exposure was reported.
Regressive cases had higher concentrations of mercury in hair indicating less impaired mercury metabolism. This indicates that children least able to excrete mercury might experience autistic symptoms immediately while regressive cases of those with some capacity to detoxify and get rid of mercury would at first appear normal, but would then build up mercury to a critical point before their excretion capacity was overwhelmed and autistic symptoms surfaced.
Gender difference in autism and mercury poisoning
Males are much more likely to be diagnosed with autism or learning and behavioral disorders, possibly due to a reduced capacity to combat oxidative stress. Interestingly, males are also more sensitive to early life mercury exposure than females. Human epidemiological studies find boys to be more susceptible to the cardiac effects of mercury. Dr. Philippe Grandjean reported effects on blood pressure and heart rate variability in Faroese boys with mercury concentrations between one and 10 µg/L (Sorensen 1999). EPA's 'safe' dose of mercury translates to approximately 5.8 µg/L. Studies of mass mercury poisoning in Minamata, Japan report a skewed birth ratio due to increased fetal death for males (Sakamoto 2001). The U.S. Centers for Disease Control found that boys had higher concentrations of mercury in hair than girls, but these differences were not statistically significant (McDowell 2004). These findings are mirrored in laboratory animals (Vahter citing Gimenez-Llort 2001).
Conclusion: The Promise of Prevention and Treatment The findings by James and her colleagues significantly strengthen the evidence of a connection between mercury and autism, but they have much broader significance for public health and pollution control policies in general. The research strongly suggests it may be possible to identify individuals susceptible to toxic chemical exposure. If confirmed, these findings would argue strongly that environmental policies designed to protect the average person from chemical exposures are grossly insufficient to protect the public health.
Public health protections from chemical pollutants commonly include a ten-fold margin of safety to account for individual differences in susceptibility. An additional ten-fold safety factor may be included to account for the increased vulnerability of children. However even this 100-fold safety factor may not account for the reduced capacity of a vulnerable child to combat oxidative stress during crucial developmental periods.
Children with the metabolic profile James has identified are very likely to be more susceptible to a vast number of common pollutants, from arsenic in drinking water and wooden play-sets, to air pollution from cars and power plants. Environmental and health officials must evaluate the adequacy of current laws and policies to protect individuals with a heightened sensitivity to chemicals exposure.
At the same time, James' work may point to a potential treatment for autistic and other children whose diseases stem from bad glutathione ratios. After identifying a common vulnerability in autistic children, Dr. James and her research partners administered micronutrients to a subset of study participants in an attempt to remedy imbalanced metabolic profiles. Children received daily supplements of glutathione precursors folinic acid (5-formyl THF) and betaine for three months, followed by methyl B12 (methyl cobalamin) for an additional month. At the end of the intervention, glutathione measurements had improved in all children (James 2004a). The physician administering the dietary intervention noted improved speech and cognition but the study was not designed to quantify the benefits. Follow-up studies are underway to include more children and document improvements in their health outcomes.
These findings raise serious concerns about the studies that have allegedly proven the safety of mercury in vaccines. While Dr. James' results do not prove that mercury in vaccinations causes autism or other neurodevelopmental disorders, they significantly strengthen that possibility by identifying a metabolic imbalance common to nearly all autistic children that would make these children poorly equipped to mount a defense against the large doses of mercury they all received via vaccines.
Oxygen radicals damage the brain and nervous system Autistic children's inability to combat oxidative stress can lead to many health problems. Oxidative stress is caused by oxygen radicals — highly unstable chemicals that react with and destroy healthy cells. These free oxygen radicals are produced by the body in manageable amounts as byproducts of normal body metabolism, but their prevalence can be exacerbated by exposure to environmental chemicals. Oxygen radicals damage cells by reacting with proteins, DNA, carbohydrates, and fats, setting off chain reactions that can only be stopped by a cell's antioxidant defense system. In the process they disrupt cell functions and interfere with signals sent between cells in the body, which can lead to auto-immunity (Klein 2003).
Oxidative damage is counteracted by the body's antioxidant systems, which convert oxygen radicals into harmless byproducts. Oxidative stress occurs when oxygen radicals overwhelm the capacity of the body's antioxidant systems. Oxidative stress affects many body systems. It damages cell membrane structure (lipids), the cell machinery that performs the essential work of the cells (proteins), and the body's ability to regulate cell growth and protein synthesis (DNA and RNA). Oxidative stress is associated with premature aging of cells, and can lead to tissue inflammation, damaged cell membranes, autoimmunity and cell death (Klein 2003). Glutathione is the most important antioxidant for metals detoxification and excretion.
The brain and nervous system are particularly vulnerable to oxidative stress due to limited antioxidant capacity. The brain makes up about two percent of a person's mass but consumes 20 percent of their metabolic oxygen. The vast majority of this energy is used by the neurons (Shulman 2004). Some brain cells, like neurons, cannot make glutathione, but instead rely on surrounding astrocyte cells to provide useable glutathione precursors. Because the brain has limited access to the bulk of antioxidants produced by the body, neurons are the first cells to be affected by a shortage of antioxidants, and are most susceptible to oxidative stress. Researchers studying antioxidant protection of neurons are finding short windows during development of high vulnerability to oxidative stress (Perry 2004).
Children are more vulnerable than adults to oxidative stress due to their naturally low glutathione levels from conception through infancy (Erden-Inal 2003, Ono 2001). Risks created by this natural deficit in detoxification capacity in infants are compounded by the fact that mercury and other environmental chemicals that invoke oxidative stress are found at higher concentrations in the developing infant than in their mothers and appear to accumulate in the placenta.
In addition to this natural variability in antioxidant status with age, a person's genes play a strong role in their ability to make antioxidants in response to oxidative stress. A host of genes determine the speed and responsiveness of antioxidant production and recycling. Some genes common in one quarter to one half of the U.S. population reduce glutathione activity and are linked with increased odds of several cancers (Hallier 1994, Engel 2002). People with gene deletions for two types of glutathione genes (GST M1 and T1) are more likely to have allergic reactions to the mercury-based preservative thimerosal (Westphal 2000).
Environmental chemicals that provoke oxidative stress could contribute to autism or other health problems During a typical day children and pregnant women are exposed to many different types of environmental chemicals that cause oxidative stress. These exposures add up, creating special concerns for infants and small children due to age-related sensitivity that derives from naturally low glutathione levels. This natural age-related vulnerability is exacerbated in individuals with impaired glutathione ratios. If these children were exposed to a high dose of any compound that produced significant oxidative stress, they would be less able to detoxify and excrete the compound.
Pervasive environmental contaminants like air pollutants from power plants and auto exhaust, pesticides, heavy metals and food additives all produce some degree of oxidative stress. Fine particulate matter and diesel exhaust both provoke tremendous oxidative stress and deplete glutathione (Li 2002). Oxygen radicals wreak havoc in the lungs of asthmatic children. The pain reliever acetaminophen and alcohol both provoke oxidative stress, but their combined effects are much more potent than either chemical alone.
Exposure to the pesticides maneb and paraquat can push neuron cells already under oxidative stress over a threshold of toxicity and "act as an additional insult to the system and prevent the normal recovery of [antioxidant] defenses" (Barlow 2005). Researchers have concluded that maneb disruptions to cells might cause neurodegeneration "especially with concurrent exposures to other environmentally relevant oxidative stressors, such as paraquat" (Barlow 2005). When they dosed pregnant mice with these pesticides the male offspring showed permanent alterations to neurological systems and enhanced susceptibility as an adult to paraquat (Barlow 2004).
PCBs induce a concentration-dependent increase in oxygen radicals. Cells with low levels of available glutathione are more sensitive to PCBs while cells pre-treated with antioxidants had reduced radical production and less cell death (Lee 2004).
Heavy metals—mercury, cadmium, chromium, cobalt, lead, antimony, nickel and others—are a major source of oxidative stress that are commonly detected in air, soil, water and food. Arsenic and chromium in pressure-treated wood, mercury in fish and vaccines, lead in paint, and metals in soil or drinking water are chronic if not daily sources of oxidative stress in the child's environment.
Glutathione is one of the bodys most important mechanism of heavy metal detoxification and excretion. Some metals—copper, chromium, iron and vanadium—directly provoke oxygen radical formation. Glutathione binds with these compounds as well as other metals—cadmium, lead, mercury, and nickel (Stohs 1995). The resulting, water-soluble chemical is more easily filtered out of the body. People with less 'active glutathione' will not be able to excrete metals as quickly. For example, cells treated with chemicals to inhibit glutathione recycling are much more sensitive to manganese toxicity (Desole 1997). People chronically exposed to arsenic in drinking water have increased oxidative damage and decreased antioxidant potential (Wu 2001).
Numerous studies link thimerosal with oxidative stress to the brain and neurological system at concentrations similar to those that were experienced by children vaccinated in the 1990s. Researchers measured mercury concentrations between 10 and 30 nanomoles per liter (nM) in premature infants given a single Hepatitis B shot at birth (Stajich 2000). Mercury concentrations ranging from 4 to 21 nM are reported in young children when measurements were collected 3 to 20 days after vaccination (Pichichero 2002). Four recent studies of thimerosal toxicity to human brain cells report oxidative damage, interruption of methylation, and decreased cell energy resulting from thimerosal exposure in the range of exposure overlapping with those for vaccinated children in the 1990s (Waly 2004, Baskin 2003, Ueha-Ishibashi 2004, Makani 2002). Several studies documented the protective benefits of antioxidants, especially glutathione, which attenuate the damages caused by thimerosal (Makani 2004, James 2005, Shanker 2003).
Impaired antioxidant production provides a common rationale for many disparate features of autistic disorders The identification of reduced antioxidant capacity as a common impairment in autistic children is an important breakthrough that should guide research into the autism epidemic. It strongly suggests that glutathione is a factor that mediates the relationship between environmental chemicals and autism, and for the first time provides a plausible biological link between several trademark features of the disorder that have baffled researchers searching for a single gene or chemical exposure that is triggering autism.
For example, scientists have failed to explain why autism rates are much higher in males, why autism manifests in some children after a period of healthy development, and why autistic children develop intestinal and autoimmune disorders at high rates. Antioxidant imbalance, particularly glutathione deficit, may be the unifying factor that links these apparently disparate symptoms and provides a clue to interventions that could treat autism. Each of these seemingly disconnected features of autism are strongly associated with glutathione capacity.
Autism rates higher, Glutathione levels lower in males
Males make up 70 percent of all autism cases, as well as the majority of children diagnosed with learning disabilities and attention deficit disorder. New research attributes weaker antioxidant capacity in young males with greater vulnerability in their brain and nervous systems, potentially effecting vulnerability to mercury and autism. Women and girls, in contrast, have lower levels of inactive antioxidant chemicals (Rush 2003). Estrogen is a powerful antioxidant that confers substantial benefits against free-radical mediated damage in aging. Male rats have four times higher rate of oxidative damage to mitochondrial DNA, which the authors pose as a reason for female's longer lifespan in many species including humans (Borrás 2003).
The difference in antioxidant capacity between males and females is most pronounced in newborns. Studies using tissue samples from newborn infants reveal significantly higher glutathione levels, glutathione production, and cell survival in response to oxidative stress in cells from girls compared to boys (Lavoie 1997). Studies of brain injury in newborns have found that inherently stronger glutathione capacity in females protects their brain cells from damage after a traumatic injury. Glutathione concentrations remain constant in females but they drop by as much as 80 percent in males after a brain injury (Du 2004). Similar studies found increased brain damage to children younger than four years old when their antioxidant systems are immature and glutathione levels are lower (Fan 2003).
Glutathione deficit may be responsible for intestinal disorders in autistic children
The reduced concentrations of glutathione Dr. James measured in study children may explain common intestinal ailments noted in autistic children. Glutathione is vital to proper functioning of the intestines. Deficits in glutathione cause degeneration of the jejunum and colon (Martensson 1990). Research suggests that oral administration of glutathione protects intestines against toxicity associated with inflammatory diseases, oxidative damage, and other toxins (Martensson 1990). Rodent studies highlight the role of glutathione in preventing positively charged substances—like metals—from passing through the gut (Samiec 2000). Laboratory studies have also demonstrated that treatment with glutathione precursors can protect the gut from different types of free-radical-mediated injury (Jefferies 2003).
Autistic children commonly suffer from intestinal disorders. In these 'leaky gut' disorders undigested proteins pass through the gut and cause oxidative damage to the brain and nervous system (White 2003). This is similar to PKU, a metabolic disorder in which the toxic accumulation of undigested phenylalanine causes oxidative damage leading to autistic-like symptoms. PKU can be averted in laboratory animals by antioxidant supplementation (Martinez-Cruz 2002). Many parents find that their autistic children's behavior and cognition improve when they eliminate milk and wheat from their diets, indicating that their inflamed intestines my be allowing the passage of undigested proteins that exacerbate their oxidative stress.
Glutathione's role in autism and auto-immunity
Autoimmune diseases are conditions in which the immune system targets the body itself instead of bacteria or other foreign objects. Autoimmunity can be triggered when genetically susceptible people are exposed to an environmental chemical or virus. Oxidative stress also plays an important role in autoimmunity by disrupting cell signaling. T lymphocytes are made less active or hypo-responsive when they are exposed to oxygen radicals. T lymphocytes regain normal responsiveness when the antioxidants N-acetyl cysteine (Cemerski 2002) and other glutathione precursors are added to the system (Hehner 2000).
A recent investigation reported chronic inflammation in the brains of autistic patients, resulting from an over-active immune system, a sign of autoimmunity (Vargas 2004). The inflammation indicates that the brain is responding to a process that is stressing or damaging brain cells, a process which might include oxygen radicals.
The weight of the evidence supports a fresh look at the mercury-autism hypothesis Both autism and mercury exposure are characterized by functional impairment to speech, language and behavior (Bernard 2001, Blaxill 2004b). Recent studies also suggest that the same key regions of the brain are affected in both cases (Limke 2004, Kates 2004). At the same time, episodes of severe mercury exposure reveal that there is no single manifestation of mercury poisoning. In fact, children exposed to high levels of mercury during gestation and infancy have suffered from strikingly different diseases.
Minamata disease resulted from in-utero exposure to mercury-contaminated fish. Children with Minamata disease had symptoms indistinguishable from mental retardation or cerebral palsy (Kondo 2000). Acrodynia resulted from mercury in infant teething powders in the early 1900s. Children with Acrodynia suffered peeling and reddened skin on their hands and feet, and heightened sensitivity to light (Warkany 1966).
Individual susceptibility played an important role in both disorders. Although thousands of children were treated with mercury-containing teething powders, only one in 500 to one in 1,000 children who were exposed developed Acrodynia (Warkany 1966). The role of individual sensitivity made it extremely difficult to link mercury exposure with what was, at the time, a new and bizarre disease. Similarly, when children have been exposed to high levels of mercury in foods, only a small group develop severe mercury poisoning while thousands are apparently unharmed (Jalili 1961, Kondo 2000).
Dr. James' findings clearly reveal a mechanism by which autistic children would be predisposed to mercury-related oxidative damage to their developing brain and nervous system. Several additional pieces of evidence strengthen the potential link between mercury exposure and autism in children with abnormal antioxidant capacity. These include:
The indisputable toxicity of mercury to the brain, particularly the developing brain (Limke 2004, Clarkson 2002, Mahaffey 1999). Peer-reviewed reports showing that autistic children are extremely poor at ridding their bodies of mercury as measured by mercury hair levels (Holmes 2003). The recent finding that autism-like symptoms are triggered by thimerosal in mice with a predisposition to autoimmunity (Hornig 2004). The fact that the prevalence of autism in boys is four times that in girls, and that boys have elevated incidence of damage from mercury exposure in epidemiologic studies (Vahter 2002). Mercury targets brain cells
Pre-natal and early life mercury exposures cause multiple impacts to basic brain development by disrupting the division and migration of neuronal cells (Mahaffey 1999). Mercury creates oxidative stress that directly kills brain cells. Human beings accumulate more mercury in the brain than in blood or other organs. Organic mercury actively transported through the blood—brain barrier accumulates in the highest concentrations in the cerebellum, especially the neuronal cells (Limke 2004). The cerebellum is the brain region associated with movement and cognition, and a key region targeted by toxic chemicals (Fonnum 2000), and a region of impairment in autistic patients (McAlonan 2004).
Dr. James investigated the effect of thimerosal on human brain astrocyte and neuron cells. She found that astrocytes have higher levels of glutathione compared to neurons and were more resistant to the cytotoxic effects of thimerosal (James 2005). Mercury was less toxic to human brain cells pretreated with glutathione or a glutathione precursor N-acetyl cysteine, which is used as a treatment for mercury intoxication and it is thought to speed mercury excretion from the body (Ballatori 1998). Similar studies have documented oxidative damages of mercury and glutathione protection to T cells, astrocytes, neurons and fibroblasts (Makani 2002, Shanker 2003).
Immune symptoms
In the summer of 2004, researchers at Columbia's Mailman School of Public Health reported symptoms similar to autism in thimerosal-exposed mice. Thimerosal was administered to three strains of laboratory mice at exposures that replicated infant exposure in the 1990s. Only the mouse strain with a predisposition to autoimmunity was affected by thimerosal exposure. These mice had significant growth delay, reduced locomotion, exaggerated response to novelty, and changes in the brain and nervous system that were suggestive of autism (Hornig 2004).
Metal metabolism and regression
Unlike most substances that are toxic to the brain, there is a significant lag time between exposure to either mercury or thimerosal, and the emergence of the symptoms of mercury poisoning. The length of the lag period depends on the severity of exposures. The delay between first exposure and on-set of symptoms of mercury poisoning has been attributed to the gradual depletion of the brain's compensatory responses, chiefly glutathione and other antioxidants (Weiss 2002).
Autism often is diagnosed after a period of seemingly healthy development. Regressive children lose previously acquired skills such as speech and mobility, or fail to progress in their development. The role that oxidative stress and environmental chemicals play in regressive autism is unknown, but studies finding reduced metal excretion in autistic children point to different dynamics in regressive autism.
A recent publication by physician Amy Holmes reported that autistic children had significantly lower levels of mercury in their hair relative to non-autistic children, suggesting greater accumulation of mercury in the body due to reduced excretion capabilities (Holmes 2003). Hair samples were analyzed from 94 autistic children and 45 non-autistic children between one and two years of age and the autistic children had significantly lower levels of mercury in their hair samples (0.47 vs. 3.63 ppm).
For non-autistic children the level of mercury in the hair sample was strongly correlated with the mother's exposure to mercury in dental fillings, fish consumption and mercury-containing RhoGAM vaccinations during pregnancy. In autistic children there was no correlation, hair levels were always low, even in cases where elevated maternal mercury exposure was reported.
Regressive cases had higher concentrations of mercury in hair indicating less impaired mercury metabolism. This indicates that children least able to excrete mercury might experience autistic symptoms immediately while regressive cases of those with some capacity to detoxify and get rid of mercury would at first appear normal, but would then build up mercury to a critical point before their excretion capacity was overwhelmed and autistic symptoms surfaced.
Gender difference in autism and mercury poisoning
Males are much more likely to be diagnosed with autism or learning and behavioral disorders, possibly due to a reduced capacity to combat oxidative stress. Interestingly, males are also more sensitive to early life mercury exposure than females. Human epidemiological studies find boys to be more susceptible to the cardiac effects of mercury. Dr. Philippe Grandjean reported effects on blood pressure and heart rate variability in Faroese boys with mercury concentrations between one and 10 µg/L (Sorensen 1999). EPA's 'safe' dose of mercury translates to approximately 5.8 µg/L. Studies of mass mercury poisoning in Minamata, Japan report a skewed birth ratio due to increased fetal death for males (Sakamoto 2001). The U.S. Centers for Disease Control found that boys had higher concentrations of mercury in hair than girls, but these differences were not statistically significant (McDowell 2004). These findings are mirrored in laboratory animals (Vahter citing Gimenez-Llort 2001).
Conclusion: The Promise of Prevention and Treatment The findings by James and her colleagues significantly strengthen the evidence of a connection between mercury and autism, but they have much broader significance for public health and pollution control policies in general. The research strongly suggests it may be possible to identify individuals susceptible to toxic chemical exposure. If confirmed, these findings would argue strongly that environmental policies designed to protect the average person from chemical exposures are grossly insufficient to protect the public health.
Public health protections from chemical pollutants commonly include a ten-fold margin of safety to account for individual differences in susceptibility. An additional ten-fold safety factor may be included to account for the increased vulnerability of children. However even this 100-fold safety factor may not account for the reduced capacity of a vulnerable child to combat oxidative stress during crucial developmental periods.
Children with the metabolic profile James has identified are very likely to be more susceptible to a vast number of common pollutants, from arsenic in drinking water and wooden play-sets, to air pollution from cars and power plants. Environmental and health officials must evaluate the adequacy of current laws and policies to protect individuals with a heightened sensitivity to chemicals exposure.
At the same time, James' work may point to a potential treatment for autistic and other children whose diseases stem from bad glutathione ratios. After identifying a common vulnerability in autistic children, Dr. James and her research partners administered micronutrients to a subset of study participants in an attempt to remedy imbalanced metabolic profiles. Children received daily supplements of glutathione precursors folinic acid (5-formyl THF) and betaine for three months, followed by methyl B12 (methyl cobalamin) for an additional month. At the end of the intervention, glutathione measurements had improved in all children (James 2004a). The physician administering the dietary intervention noted improved speech and cognition but the study was not designed to quantify the benefits. Follow-up studies are underway to include more children and document improvements in their health outcomes.
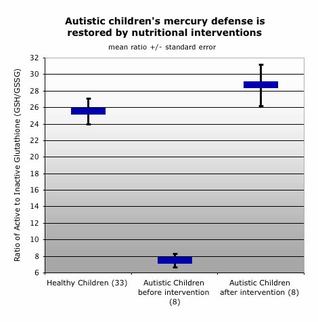
Glutathione and antioxidant precursors have been examined as treatments for metabolic conditions like PKU that create long-term oxidative stress (Baielli 2003). A small pilot study found that glutathione supplements caused a 42 percent decline in disability for patients with Parkinson's disease (Sechi 1996). Antioxidants are also proposed to treat metal toxicity, particularly arsenic (Flora 1999), borate (Banner 1986), cadmium (Tandon 2003), chromate (Banner 1986), copper (Henderson 1985), lead (Tandon 2003), and mercury (Ballatori 1998).
Oxidative damage to brain cells during pregnancy and early life can lead to permanent changes to brain structure and functioning, resulting in autism. In order to fully protect brain cells, glutathione and antioxidant precursors must be administered in advance of environmental exposures that stress or kill brain cells. Nonetheless, bolstering glutathione recycling in children already diagnosed with autism could ameliorate many downstream effects of glutathione depletion including intestinal function, auto-immunity, and cellular inflammation. Dr. James is hopeful that the success of the intervention "implies that certain aspects of autism may be treatable" (James 2004a).
References American Academy of Pediatrics, Center for Disease Control's National Center on Birth Defects and Developmental Disabilities. 2004. Autism A.L.A.R.M. http://www.medicalhomeinfo.org
Autism Society of America. 2003. Autism Cost to Economy in Billions. Available at: http://www.autism-society.org/site/
News2?JServSessionIdr008=qsr4rlqyt1.app26a&page=NewsArticle&id=5828
Baieli S, Pavone L, Meli C, Fiumara A, Coleman M. 2003. Autism and phenylketonuria. J Autism Dev Disord. 33(2):201-4.
Ballatori N, Lieberman MW, Wang W. 1998. N-acetylcysteine as an antidote in methylmercury poisoning. Environ Health Perspect. 106(5):267-71.
Banner W Jr, Koch M, Capin DM, Hopf SB, Chang S, Tong TG. 1986. Experimental chelation therapy in chromium, lead, and boron intoxication with N-acetylcysteine and other compounds. Toxicol Appl Pharmacol. 83(1):142-7.
Barclay L. 2004. Mercury Linked to Autism-Like Damage in Mice: Institute of Medicine Says Study Does Not Support Link Between Mercury, Autism in Humans. WebMD Medical News. June 9, 2004. Available at: http://my.webmd.com/content/Article/88/99936.htm
Barlow BK 2004. A fetal risk factor for Parkinson's disease. Dev Neurosci. 26(1):11-23.
Barlow BK, Lee DW, Cory-Slechta DA, Opanashuk LA. 2005. Modulation of antioxidant defense systems by the environmental pesticide maneb in dopaminergic cells. Neurotoxicology. 26(1):63-75.
Baskin DS, Ngo H, Didenko VV. 2003. Thimerosal induces DNA breaks, caspase-3 activation, membrane damage, and cell death in cultured human neurons and fibroblasts. Tox Sci 74(2):361-8.
Bernard S. 2001. Autism: a novel form of mercury poisoning. Medical Hypotheses 56(4):462-471.
Blaxill M. 2001. Presentation to Immunization Safety Review Committee. Rising Incidence of Autism: Association with Thimerosal. Cambridge, Massachusetts. July 16, 2001. Available at: www.iom.edu/includes/DBFile.asp?id=7505
Blaxill M. 2004a. What's Going On? The Question of Time Trends in Autism. Public Health Reports. (119)536-551.
Blaxill M, Redwood L, Bernard S. 2004b. Thimerosal and autism? A plausible hypothesis that should not be dismissed. Medical Hypotheses. (62)788-94.
Borras C, Sastre J, Garcia Sala D, Lloret A, Pallardo FV, Vina J. 2003. Mitochondria from females exhibit higher antioxidant gene expression and lower oxidative damage than males. Free Radical Biology & Medicine. 34(5):546-52.
Cemerski S. 2002. Reactive Oxygen Species Differentially Affect T Cell Receptor-signaling Pathways. Journal of Biological Chemistry. 227(22):19585-92.
Centers for Disease Control. 1995. Recommended Childhood Immunization Schedule -- United States, 1995. http://www.cdc.gov/mmwr/preview/mmwrhtml/00038256.htm Last reviewed May 2001.
Centers for Disease Control. 2004. Questions & Answers: Thimerosal-Containing Influenza Vaccine. http://www.cdc.gov/flu/about/qa/thimerosal.htm Updated October 26, 2004.
Chrysochoou C. 2003. An 11-month-old boy with psychomotor regression and auto-aggressive behaviour. Eur J Pediatr. (162):559-561.
Clarkson TW. 2002. Three modern faces of mercury. Environmental Health Perspectives. 110(Suppl 1):11-23.
Croen LA, Grether JK. 2003. A Response to Blaxill, Baskin, and Spitzer on Croen et al. (2002), 'The Changing Prevalence of Autism in California.' Journal of Autism and Developmental Disorders, 33(2):227-9.
Desole MS, Esposito G, Migheli R, Sircana S, Delogu MR, Fresu L, Miele M, de Natale G, Miele E. 1997. Glutathione deficiency potentiates manganese toxicity in rat striatum and brainstem and in PC12 cells. Pharmacol Res. 36(4):285-92.
Du L, Bayir H, Lai Y, Zhang X, Kochanek PM, Watkins SC, Graham SH, Clark RS. 2004. Innate gender-based proclivity in response to cytotoxicity and programmed cell death pathway. J Biol Chem. 279(37):38563-70.
Engel LS. 2002. Pooled analysis and meta-analysis of Glutathione S-Transferase M1 and Bladder Cancer: a HuGE review. Am J Epidemiol (156):95-109.
Erden-Inal M, Sunal E, Kanbak G. 2002. Age-related changes in the glutathione redox system. Cell Biochem Funct. 20(1):61-6.
Fan P, Yamauchi T, Noble LJ, Ferriero DM. 2003. Age-Dependent Differences in Glutathione Peroxidase Activity After Traumatic Brain Injury. Journal of Neurotrauma. 20(5):437-445.
Flora SJ. 1999. Arsenic-induced oxidative stress and its reversibility following combined administration of N-acetylcysteine and meso 2,3-dimercaptosuccinic acid in rats. Clin Exp Pharmacol Physiol. 26(11):865-9.
Fonnum F, Lock EA. 2000. Cerebellum as a target for toxic substances. Toxicol Lett. (112-113):9-16.
Food and Drug Administration, Center for Biologics Evaluation and Research. 2004a. Mercury in Plasma-Derived Products. http://www.fda.gov/cber/blood/mercplasma.htm Updated September 9, 2004
FDA Center for Biologics Evaluation and Research. 2004b. Mercury in Vaccines http://www.fda.gov/cber/vaccine/thimerosal.htm Updated September 28, 2004.
Gimenez-Llort L, Ahlbom E, Dare E, Vahter M, Ogren S, Ceccatelli S. 2001. Prenatal exposure to methylmercury changes dopamine-modulated motor activity during early ontogeny: age and gender-dependent effects. Environ. Toxicol. Pharmacol. 9(3):61-70.
Granot E, Kohen R. 2004. Oxidative stress in childhood health and disease states. Clinical Nutrition 23(1):3-11.
Hallier E, Schroder KR, Asmuth K, Dommermuth A, Aust B, Goergens HW. 1994. Metabolism of dichloromethane (methylene chloride) to formaldehyde in human erythrocytes: influence of polymorphism of glutathione transferase theta (GST T1-1). Arch Toxicol. 68(7):423-7.
Hehner SP. 2000. Enhancement of T cell receptor signaling by a mild oxidative shift in the intracellular thiol pool. J. Immunol. 165(8):4319-4328.
Henderson P, Hale TW, Shum S, Habersang RW. 1985. N-Acetylcysteine therapy of acute heavy metal poisoning in mice.Vet Hum Toxicol. 27(6):522-5.
Holmes AS, Blaxill MF, Haley BE. 2003. Reduced Levels of Mercury in First Baby Haircuts of Autistic Children. International Journal of Toxicology, (22):277-285.
Hornig M, Chian D, Lipkin WI. 2004. Neurotoxic effects of postnatal thimerosal are mouse strain dependent. Mol Psychiatry. 9(9):833-45.
Institute of Medicine. 2004a. Press Release: MMR Vaccine and Thimerosal-Containing Vaccines Are Not Associated With Autism, IOM Report Says. May 18, 2004. http://www4.nationalacademies.org/news.nsf/isbn/030909237X?OpenDocument
Institute of Medicine. 2004b. Immunization Safety Review: Vaccines and Autism. National Academies Press. Available at: http://books.nap.edu/catalog/10997.html
Jalili MA, Abbasi AH. 1961. Poisoning by ethyl mercury toluene sulphonanilide. Br J Ind Med. (18):303-8.
James SJ, Cutler P, Melnyk S, Hernigan S, Janak L, Gaylor DW, Neubrander JA. 2004a. Metabolic biomarkers of increased oxidative stress and methylation capacity in children with autism. American Journal of Clinical Nutrition. 80(6):1611-1617. [Advanced copy available at http://www.ajcn.org/cgi/content/full/80/6/1611]
James SJ, et al. 2004b. Unpublished results follow-up testing of 75 autistic children and 42 controls. Personal communication with EWG.
James SJ, Slikker W 3rd, Melnyk S, New E, Pogribna M, Jernigan S. 2005. Thimerosal Neurotoxicity is Associated with Glutathione Depletion: Protection with Glutathione Precursors. Neurotoxicology. 26(1):1-8.
Jefferies H. 2003. The role of glutathione in intestinal dysfunction. J Invest Surg. 16(6):315-23.
Kates WR, Burnette CP, Eliez S, Strunge LA, Kaplan D, Landa R, Reiss AL, Pearlson GD. 2004. Neuroanatomic variation in monozygotic twin pairs discordant for the narrow phenotype for autism. Am J Psychiatry. 161(3):539-46.
Klein JA, Ackerman SL. 2003. Oxidative stress, cell cycle, and neurodegeneration. In Redox Signaling in Biology and Disease, Roy J. Soberman, Series Editor J. Clin. Invest. (111):785-793.
Kondo K. 2000. Congenital Minamata disease: warning from Japan's experience. J Child Neurol. 15(7):458-64.
Lavoie JC, Chessex P. 1997. Gender and maturation affect glutathione statues in human neonatal tissues. Free Radical Biology & Medicine. 23(4)648-57.
Lee DW, Opanashuk LA. 2004. Polychlorinated biphenyl mixture aroclor 1254-induced oxidative stress plays a role in dopaminergic cell injury. Neurotoxicology. 25(6):925-39.
Levin. 2004. 'Taking It to Vaccine Court; Parents say mercury in shots caused their children's autism, and they want drug firms to pay. The industry calls its defense rock-solid.' Los Angeles Times, August 7, 2004. Foreign Desk; Part A; Pg. 1.
Li N, Kim S, Wang M, Froines J, Sioutas C, Nel A. 2002. Use of a stratified oxidative stress model to study the biological effects of ambient concentrated and diesel exhaust particulate matter. Inhal Toxicol. 14(5):459-86.
Limke TL, Heidemann SF, Atchison WD. 2004. Disruption of intraneuronal divalent cation regulation by methylmercury: are specific targets involved in altered neuronoal development and cytotoxicity in methylmercury poisoning? NeruroToxicology. (25):741-60.
London E, Etzel RA. 2000. The environment as an etiologic factor in autism: A new direction for research. Environmental Health Perspectives. (108)S3.
Mahaffey KR. 1999. Methylmercury: A new look at the risks. Public Health Reports. 114(5):402-13.
Mahaffey KR. 2004. Methylmercury: Epidemiology Update. Slide presentation given at the National Forum on Contaminants in Fish. San Diego, CA. January 26, 2004. http://www.epa.gov/waterscience/fish/forum/2004/
presentations/monday/mahaffey.pdf Accessed November 29, 2004.
Makani S. 2002. Biochemical and molecular basis of thimerosal-induced apoptosis in T cells: a major role of mitochondrial pathway. Genes and Immunity 3(5)270-278.
Martensson J. 1990. Glutathione is required for intestinal function. Proc. Natl. Acad. Sci. (87):1715-19.
Martinez-Cruz F, Pozo D, Osuna C, Espinar A, Marchante C, Guerrero JM. 2002. Oxidative stress induced by phenylketonuria in the rat: Prevention by melatonin, vitamin E, and vitamin C. J Neurosci Res. 69(4):550-8.
McAlonan GM, Cheung V, Cheung C, Suckling J, Lam GY, Tai KS, Yip L, Murphy DG, Chua SE. 2004. Mapping the brain in autism. A voxel-based MRI study of volumetric differences and intercorrelations in autism. Brain. (0):3321.
McCormick MC. 2001. Opening Statement, Institute of Medicine News Conference on the Institute of Medicine Report on Thimerosal and Neurodevelopmental Outcomes, October 2001. Available at: http://www.cdc.gov/nip/news/iom-thim-stmt-10-1-01.htm
McDowell MA, Dillon CF, Osterloh J, Bolger PM, Pellizzari E, Fernando R, Montes de Oca R, Schober SE, Sinks T, Jones RL, Mahaffey KR. 2004. Hair mercury levels in U.S. children and women of childbearing age: reference range data from NHANES 1999-2000. Environ Health Perspect. 112(11):1165-7.
Ono H. 2001. Plasma total glutathione concentrations in healthy pediatric and adult subjects. Clin Chim Acta. 312(1-2):227-9.
Perry SW, Norman JP, Litzburg A, Gelbard HA. 2004. Antioxidants are required during the early critical period, but not later, for neuronal survival. J Neurosci Res. 78(4):485-92.
Pichichero ME, Cernichiari E, Lopreiato J, Treanor J.Mercury concentrations and metabolism in infants receiving vaccines containing thiomersal: a descriptive study. Lancet. 360(9347):1737-41.
Ristoff E, Larsson A. 2002. Oxidative stress in inborn errors of metabolism: Lessons from glutathione deficiency. J Inherit Metab Dis. (25):223-226.
Rush JW, Sandiford SD. 2003. Plasma glutathione peroxidase in healthy young adults: influence of gender and physical activity. Clin Biochem. 36(5):345-51.
Sakamoto M, Nakano A, Akagi H. 2001. Declining Minamata male birth ratio associated with increased male fetal death due to heavy methylmercury pollution. Environ. Res. (87):92-98.
Samiec PS. 2000. Glutathione S-Transferase in Mucus of Rat Small Intestine. Tox Sci (54):52-59.
Schulz JB, Lindenau J, Seyfried J, Dichgans J. 2000. Glutathione, oxidative stress and neurodegeneration. Eur. J. Biochem. (267)4904-11.
Shanker G, Aschner M. 2003. Methylmercury-induced reactive oxygen species formation in neonatal cerebral astrocytic cultures is attenuated by antioxidants. Molecular Brain Research. (110):85-91.
Shulman RG, Rothman DL, Behar KL, Hyder F. 2004. Energetic basis of brain activity: implications for neuroimaging. Trends Neurosci. 27(8):489-95.
Skullerud K, Marstein S,Schrader H,Brunde let PJ, Jellum E. 1980. The cerebral lesions in a patient with generalized glutathione deficiency and pyroglutamic aciduria (5-oxoprolinuria). Acta Neuropathol (52):235-238.
Sorensen N, Murata K, Butz-Jorgensen E, Weihe P, Grandjean P. 1999. Prenatal methylmercury exposure as a cardiovascular risk factor at seven years of age. Epidemiology. 10(4):370-5.
Stajich GV, Lopez GP, Harry SW, Sexson WR. 2000. Iatrogenic exposure to mercury after hepatitis B vaccination in preterm infants. J Pediatr. 136(5):679-81.
Stohs SJ, Bagchi D. 1995. Oxidative mechanisms in the toxicity of metal ions. Free Radical Biology & Medicine. 18(2)321-336.
Tandon SK, Singh S, Prasad S, Khandekar K, Dwivedi VK, Chatterjee M, Mathur N. 2003. Reversal of cadmium induced oxidative stress by chelating agent, antioxidant or their combination in rat. Toxicol Lett. 10(145)3:211-7.
Ueha-Ishibashi T, Oyama Y, Nakao H, Umebayashi C, Nishizaki Y, Tatsuishi T, Iwase K, Murao K, Seo H. 2004. Effect of thimerosal, a preservative in vaccines, on intracellular Ca(2+) concentration of rat cerebellar neurons. Toxicology. 195(1):77-84.
Vahter M, Berglund M, Akesson A, Liden C. 2002. Metals and Women's Health. Environmental Research Section A. (88):145-55.
Vargas D. 2004. Neuroglial activation and neuroinflammation in the brain of patients with autism. Annals of Neurology. DOI: 10.1002/ana.20315
Verstraeten T. 2004. Thimerosal, the Centers for Disease Control and Prevention, and GlaxoSmithKline. Pediatrics. 113(4):932.
Waly M, Olteanu H, Banerjee R, Choi SW, Mason JB, Parker BS, Sukumar S, Shim S, Sharma A, Benzecry JM, Power-Charnitsky VA, Deth RC. 2004. Activation of methionine synthase by insulin-like growth factor-1 and dopamine: a target for neurodevelopmental toxins and thimerosal. Mol Psychiatry 9(4):358-70.
Warkany J. 1966. Acrodynia - postmortem of a disease. Am J Dis Child (112):147-156.
Weiss B, Clarkson TW, Simon W. 2002. Silent latency periods in methylmercury poisoning and in neurodegenerative disease. Environ Health Perspect. 110(Suppl 5):851-4.
Westphal GA, Schnuch A, Schulz TG, Reich K, Aberer W, Brasch J, Koch P, Wessbecher R, Szliska C, Bauer A, Hallier E. 2000. Homozygous gene deletions of the glutathione S-transferases M1 and T1 are associated with thimerosal sensitization. Int Arch Occup Environ Health. 73(6):384-8.
White JF. 2003. Intestinal Pathophysiology in Autism. Society for Experimental Biology and Medicine. 228(6):639-49.
Wu MM, Chiou HY, Wang TW, Hsueh YM, Wang IH, Chen CJ, Lee TC. 2001. Association of blood arsenic levels with increased reactive oxidants and decreased antioxidant capacity in a human population of northeastern Taiwan. Environ Health Perspect. 109(10):1011-7.
Hidden Asthma Triggers
Research reveals two common culprits
by Teri Walsh
http://msn.prevention.com/article/0,5778,s2-1-77-18-353-1,00.html
A common pain reliever--or a glass of wine--could bring on an asthma attack, two studies suggest.
The first study looked at the effect of acetaminophen on 1,574 people, 664 of whom had asthma. (Acetaminophen is an active ingredient contained in Tylenol and other non-aspirin pain relievers.) Researchers found that the more acetaminophen that people with asthma took, the more often they woke up at night with symptoms and the worse their reported quality of life (Thorax, Apr 2000).
The reason: Acetaminophen may deplete an essential antioxidant in the lungs called glutathione, says lead study author Seif Shaheen, MD, PhD, researcher and senior lecturer at Guy's, King's and St. Thomas' School of Medicine, King's College, London.
The second study examined the effect of food and drink on 336 asthmatics. Researchers found that one-third believed that alcohol--especially red or white wine--made symptoms worse (The Jour. of Allergy and Clinical Immunology, Mar 2000). Evidence suggests that sulfite preservatives, histamines, or salicylates may be responsible, rather than the alcohol itself, says lead study author Hassan Vally, research scientist at the Asthma and Allergy Research Institute, Inc., in Nedlands, Western Australia.
Tylenol decreases glutathion. Many of us (myself included) foolishly gave our kids Tylenol after (and sometimes even before) vaccinating at the direction of our pediatricians to minimize the negative side effects of the vaccines (like fever, crankiness, etc). My oldest son was vaccinated through age 2 and had tylenol OFTEN after vaccines as well as all of the times he was sick (which was almost constantly following his MMR). His lab results showed that he had virtually NO glutathion. My youngest was vaccinated through age 5 mos and almost never had tylenol (maybe 2x in his whole life through age 4) and his glutathion levels were very good. Just
one more reason I could kick myself for the rest of my life. No time, got to move on, think positive and heal my kids. Below is info on the importance of glutathion from TACA's website:
Glutathione helps to defend the body against damage from cigarette smoking, exposure to radiation, cancer chemotherapy, and toxins such as alcohol. As a detoxifier of heavy metals and drugs, it aids in the treatment of blood and liver disorders. Glutathione protects cells in several ways. It neutralizes oxygen molecules
before they can harm cells. Together with selenium, it forms the enzyme glutathione peroxidase, which neutralizes hydrogen peroxide. It is also a component of another antioxidant enzyme, glutathione-S-transferase, which is a broad-spectrum liver-detoxifying enzyme.
Glutathione protects not only individual cells but also the tissues of the arteries, brain, heart, immune cells, kidneys, lenses of the eyes, liver, lungs, and skin against oxidant damage. It plays a role in preventing cancer, especially liver cancer, and may also have an anti-aging effect. Glutathione can be taken in supplement form. The production of glutathione by the body can be boosted by taking supplemental N-acetylcysteine or L-cysteine plus L-methionine. Studies suggest that this may be a better way or raising glutathione levels than taking glutathione itself. Glutathione is not technically an amino acid, however, due to its close relationship is normally grouped with the amino acids. Most glutathione is found in the liver where it detoxifies many harmful compounds to be excreted thru the bile. Some glutathione is released directly by the liver into the bloodstream where it helps to maintain the strength of your red blood cells and also protecting your white blood cells.
Glutathione can also be found in the lungs and in your body's intestinal tract system. It is required for carbohydrate metabolism. Glutathione also appears to have anti-aging effects by aiding in the breakdown of oxidized fats that may contribute to atherosclerosis. As we get older glutathione levels in the body get lower and this can cause an increase in the aging process. Thus glutathione supplementation is useful to prevent this from occurring. Glutathione deficiency maybe indicated by: coordination problems, mental disorder, tremors, twitching, nervous system disorder, and difficulty in balancing. Currently, believed to be caused by lesions in the brain.
Severity of Autism Is Associated With Toxic Metal Body Burden and Red Blood Cell Glutathione Levels
Adams J et al
Journal of Toxicology
Provisional PDF:
http://www.hindawi.com/journals/jt/aip.532640.pdf
Abstract: This study investigated the relationship of children’s autism symptoms with their toxic metal body burden and red blood cell (RBC) glutathione levels. In children ages 3-8 years, the severity of autism was assessed using four tools: ADOS, PDD-BI, ATEC, and SAS. Toxic metal body burden was assessed by measuring urinary excretion of toxic metals, both before and after oral dimercaptosuccinic acid (DMSA). Multiple positive correlations were found between the severity of autism and the urinary excretion of toxic metals. Variations in the severity of autism measurements could be explained, in part, by regression analyses of urinary excretion of toxic metals before and after DMSA and the level of RBC glutathione (adjusted R2 of 0.22-0.45, p<0.005 in all cases). This study demonstrates a significant positive association between the severity of autism and the relative body burden of toxic metals.
Oxidative damage to brain cells during pregnancy and early life can lead to permanent changes to brain structure and functioning, resulting in autism. In order to fully protect brain cells, glutathione and antioxidant precursors must be administered in advance of environmental exposures that stress or kill brain cells. Nonetheless, bolstering glutathione recycling in children already diagnosed with autism could ameliorate many downstream effects of glutathione depletion including intestinal function, auto-immunity, and cellular inflammation. Dr. James is hopeful that the success of the intervention "implies that certain aspects of autism may be treatable" (James 2004a).
References American Academy of Pediatrics, Center for Disease Control's National Center on Birth Defects and Developmental Disabilities. 2004. Autism A.L.A.R.M. http://www.medicalhomeinfo.org
Autism Society of America. 2003. Autism Cost to Economy in Billions. Available at: http://www.autism-society.org/site/
News2?JServSessionIdr008=qsr4rlqyt1.app26a&page=NewsArticle&id=5828
Baieli S, Pavone L, Meli C, Fiumara A, Coleman M. 2003. Autism and phenylketonuria. J Autism Dev Disord. 33(2):201-4.
Ballatori N, Lieberman MW, Wang W. 1998. N-acetylcysteine as an antidote in methylmercury poisoning. Environ Health Perspect. 106(5):267-71.
Banner W Jr, Koch M, Capin DM, Hopf SB, Chang S, Tong TG. 1986. Experimental chelation therapy in chromium, lead, and boron intoxication with N-acetylcysteine and other compounds. Toxicol Appl Pharmacol. 83(1):142-7.
Barclay L. 2004. Mercury Linked to Autism-Like Damage in Mice: Institute of Medicine Says Study Does Not Support Link Between Mercury, Autism in Humans. WebMD Medical News. June 9, 2004. Available at: http://my.webmd.com/content/Article/88/99936.htm
Barlow BK 2004. A fetal risk factor for Parkinson's disease. Dev Neurosci. 26(1):11-23.
Barlow BK, Lee DW, Cory-Slechta DA, Opanashuk LA. 2005. Modulation of antioxidant defense systems by the environmental pesticide maneb in dopaminergic cells. Neurotoxicology. 26(1):63-75.
Baskin DS, Ngo H, Didenko VV. 2003. Thimerosal induces DNA breaks, caspase-3 activation, membrane damage, and cell death in cultured human neurons and fibroblasts. Tox Sci 74(2):361-8.
Bernard S. 2001. Autism: a novel form of mercury poisoning. Medical Hypotheses 56(4):462-471.
Blaxill M. 2001. Presentation to Immunization Safety Review Committee. Rising Incidence of Autism: Association with Thimerosal. Cambridge, Massachusetts. July 16, 2001. Available at: www.iom.edu/includes/DBFile.asp?id=7505
Blaxill M. 2004a. What's Going On? The Question of Time Trends in Autism. Public Health Reports. (119)536-551.
Blaxill M, Redwood L, Bernard S. 2004b. Thimerosal and autism? A plausible hypothesis that should not be dismissed. Medical Hypotheses. (62)788-94.
Borras C, Sastre J, Garcia Sala D, Lloret A, Pallardo FV, Vina J. 2003. Mitochondria from females exhibit higher antioxidant gene expression and lower oxidative damage than males. Free Radical Biology & Medicine. 34(5):546-52.
Cemerski S. 2002. Reactive Oxygen Species Differentially Affect T Cell Receptor-signaling Pathways. Journal of Biological Chemistry. 227(22):19585-92.
Centers for Disease Control. 1995. Recommended Childhood Immunization Schedule -- United States, 1995. http://www.cdc.gov/mmwr/preview/mmwrhtml/00038256.htm Last reviewed May 2001.
Centers for Disease Control. 2004. Questions & Answers: Thimerosal-Containing Influenza Vaccine. http://www.cdc.gov/flu/about/qa/thimerosal.htm Updated October 26, 2004.
Chrysochoou C. 2003. An 11-month-old boy with psychomotor regression and auto-aggressive behaviour. Eur J Pediatr. (162):559-561.
Clarkson TW. 2002. Three modern faces of mercury. Environmental Health Perspectives. 110(Suppl 1):11-23.
Croen LA, Grether JK. 2003. A Response to Blaxill, Baskin, and Spitzer on Croen et al. (2002), 'The Changing Prevalence of Autism in California.' Journal of Autism and Developmental Disorders, 33(2):227-9.
Desole MS, Esposito G, Migheli R, Sircana S, Delogu MR, Fresu L, Miele M, de Natale G, Miele E. 1997. Glutathione deficiency potentiates manganese toxicity in rat striatum and brainstem and in PC12 cells. Pharmacol Res. 36(4):285-92.
Du L, Bayir H, Lai Y, Zhang X, Kochanek PM, Watkins SC, Graham SH, Clark RS. 2004. Innate gender-based proclivity in response to cytotoxicity and programmed cell death pathway. J Biol Chem. 279(37):38563-70.
Engel LS. 2002. Pooled analysis and meta-analysis of Glutathione S-Transferase M1 and Bladder Cancer: a HuGE review. Am J Epidemiol (156):95-109.
Erden-Inal M, Sunal E, Kanbak G. 2002. Age-related changes in the glutathione redox system. Cell Biochem Funct. 20(1):61-6.
Fan P, Yamauchi T, Noble LJ, Ferriero DM. 2003. Age-Dependent Differences in Glutathione Peroxidase Activity After Traumatic Brain Injury. Journal of Neurotrauma. 20(5):437-445.
Flora SJ. 1999. Arsenic-induced oxidative stress and its reversibility following combined administration of N-acetylcysteine and meso 2,3-dimercaptosuccinic acid in rats. Clin Exp Pharmacol Physiol. 26(11):865-9.
Fonnum F, Lock EA. 2000. Cerebellum as a target for toxic substances. Toxicol Lett. (112-113):9-16.
Food and Drug Administration, Center for Biologics Evaluation and Research. 2004a. Mercury in Plasma-Derived Products. http://www.fda.gov/cber/blood/mercplasma.htm Updated September 9, 2004
FDA Center for Biologics Evaluation and Research. 2004b. Mercury in Vaccines http://www.fda.gov/cber/vaccine/thimerosal.htm Updated September 28, 2004.
Gimenez-Llort L, Ahlbom E, Dare E, Vahter M, Ogren S, Ceccatelli S. 2001. Prenatal exposure to methylmercury changes dopamine-modulated motor activity during early ontogeny: age and gender-dependent effects. Environ. Toxicol. Pharmacol. 9(3):61-70.
Granot E, Kohen R. 2004. Oxidative stress in childhood health and disease states. Clinical Nutrition 23(1):3-11.
Hallier E, Schroder KR, Asmuth K, Dommermuth A, Aust B, Goergens HW. 1994. Metabolism of dichloromethane (methylene chloride) to formaldehyde in human erythrocytes: influence of polymorphism of glutathione transferase theta (GST T1-1). Arch Toxicol. 68(7):423-7.
Hehner SP. 2000. Enhancement of T cell receptor signaling by a mild oxidative shift in the intracellular thiol pool. J. Immunol. 165(8):4319-4328.
Henderson P, Hale TW, Shum S, Habersang RW. 1985. N-Acetylcysteine therapy of acute heavy metal poisoning in mice.Vet Hum Toxicol. 27(6):522-5.
Holmes AS, Blaxill MF, Haley BE. 2003. Reduced Levels of Mercury in First Baby Haircuts of Autistic Children. International Journal of Toxicology, (22):277-285.
Hornig M, Chian D, Lipkin WI. 2004. Neurotoxic effects of postnatal thimerosal are mouse strain dependent. Mol Psychiatry. 9(9):833-45.
Institute of Medicine. 2004a. Press Release: MMR Vaccine and Thimerosal-Containing Vaccines Are Not Associated With Autism, IOM Report Says. May 18, 2004. http://www4.nationalacademies.org/news.nsf/isbn/030909237X?OpenDocument
Institute of Medicine. 2004b. Immunization Safety Review: Vaccines and Autism. National Academies Press. Available at: http://books.nap.edu/catalog/10997.html
Jalili MA, Abbasi AH. 1961. Poisoning by ethyl mercury toluene sulphonanilide. Br J Ind Med. (18):303-8.
James SJ, Cutler P, Melnyk S, Hernigan S, Janak L, Gaylor DW, Neubrander JA. 2004a. Metabolic biomarkers of increased oxidative stress and methylation capacity in children with autism. American Journal of Clinical Nutrition. 80(6):1611-1617. [Advanced copy available at http://www.ajcn.org/cgi/content/full/80/6/1611]
James SJ, et al. 2004b. Unpublished results follow-up testing of 75 autistic children and 42 controls. Personal communication with EWG.
James SJ, Slikker W 3rd, Melnyk S, New E, Pogribna M, Jernigan S. 2005. Thimerosal Neurotoxicity is Associated with Glutathione Depletion: Protection with Glutathione Precursors. Neurotoxicology. 26(1):1-8.
Jefferies H. 2003. The role of glutathione in intestinal dysfunction. J Invest Surg. 16(6):315-23.
Kates WR, Burnette CP, Eliez S, Strunge LA, Kaplan D, Landa R, Reiss AL, Pearlson GD. 2004. Neuroanatomic variation in monozygotic twin pairs discordant for the narrow phenotype for autism. Am J Psychiatry. 161(3):539-46.
Klein JA, Ackerman SL. 2003. Oxidative stress, cell cycle, and neurodegeneration. In Redox Signaling in Biology and Disease, Roy J. Soberman, Series Editor J. Clin. Invest. (111):785-793.
Kondo K. 2000. Congenital Minamata disease: warning from Japan's experience. J Child Neurol. 15(7):458-64.
Lavoie JC, Chessex P. 1997. Gender and maturation affect glutathione statues in human neonatal tissues. Free Radical Biology & Medicine. 23(4)648-57.
Lee DW, Opanashuk LA. 2004. Polychlorinated biphenyl mixture aroclor 1254-induced oxidative stress plays a role in dopaminergic cell injury. Neurotoxicology. 25(6):925-39.
Levin. 2004. 'Taking It to Vaccine Court; Parents say mercury in shots caused their children's autism, and they want drug firms to pay. The industry calls its defense rock-solid.' Los Angeles Times, August 7, 2004. Foreign Desk; Part A; Pg. 1.
Li N, Kim S, Wang M, Froines J, Sioutas C, Nel A. 2002. Use of a stratified oxidative stress model to study the biological effects of ambient concentrated and diesel exhaust particulate matter. Inhal Toxicol. 14(5):459-86.
Limke TL, Heidemann SF, Atchison WD. 2004. Disruption of intraneuronal divalent cation regulation by methylmercury: are specific targets involved in altered neuronoal development and cytotoxicity in methylmercury poisoning? NeruroToxicology. (25):741-60.
London E, Etzel RA. 2000. The environment as an etiologic factor in autism: A new direction for research. Environmental Health Perspectives. (108)S3.
Mahaffey KR. 1999. Methylmercury: A new look at the risks. Public Health Reports. 114(5):402-13.
Mahaffey KR. 2004. Methylmercury: Epidemiology Update. Slide presentation given at the National Forum on Contaminants in Fish. San Diego, CA. January 26, 2004. http://www.epa.gov/waterscience/fish/forum/2004/
presentations/monday/mahaffey.pdf Accessed November 29, 2004.
Makani S. 2002. Biochemical and molecular basis of thimerosal-induced apoptosis in T cells: a major role of mitochondrial pathway. Genes and Immunity 3(5)270-278.
Martensson J. 1990. Glutathione is required for intestinal function. Proc. Natl. Acad. Sci. (87):1715-19.
Martinez-Cruz F, Pozo D, Osuna C, Espinar A, Marchante C, Guerrero JM. 2002. Oxidative stress induced by phenylketonuria in the rat: Prevention by melatonin, vitamin E, and vitamin C. J Neurosci Res. 69(4):550-8.
McAlonan GM, Cheung V, Cheung C, Suckling J, Lam GY, Tai KS, Yip L, Murphy DG, Chua SE. 2004. Mapping the brain in autism. A voxel-based MRI study of volumetric differences and intercorrelations in autism. Brain. (0):3321.
McCormick MC. 2001. Opening Statement, Institute of Medicine News Conference on the Institute of Medicine Report on Thimerosal and Neurodevelopmental Outcomes, October 2001. Available at: http://www.cdc.gov/nip/news/iom-thim-stmt-10-1-01.htm
McDowell MA, Dillon CF, Osterloh J, Bolger PM, Pellizzari E, Fernando R, Montes de Oca R, Schober SE, Sinks T, Jones RL, Mahaffey KR. 2004. Hair mercury levels in U.S. children and women of childbearing age: reference range data from NHANES 1999-2000. Environ Health Perspect. 112(11):1165-7.
Ono H. 2001. Plasma total glutathione concentrations in healthy pediatric and adult subjects. Clin Chim Acta. 312(1-2):227-9.
Perry SW, Norman JP, Litzburg A, Gelbard HA. 2004. Antioxidants are required during the early critical period, but not later, for neuronal survival. J Neurosci Res. 78(4):485-92.
Pichichero ME, Cernichiari E, Lopreiato J, Treanor J.Mercury concentrations and metabolism in infants receiving vaccines containing thiomersal: a descriptive study. Lancet. 360(9347):1737-41.
Ristoff E, Larsson A. 2002. Oxidative stress in inborn errors of metabolism: Lessons from glutathione deficiency. J Inherit Metab Dis. (25):223-226.
Rush JW, Sandiford SD. 2003. Plasma glutathione peroxidase in healthy young adults: influence of gender and physical activity. Clin Biochem. 36(5):345-51.
Sakamoto M, Nakano A, Akagi H. 2001. Declining Minamata male birth ratio associated with increased male fetal death due to heavy methylmercury pollution. Environ. Res. (87):92-98.
Samiec PS. 2000. Glutathione S-Transferase in Mucus of Rat Small Intestine. Tox Sci (54):52-59.
Schulz JB, Lindenau J, Seyfried J, Dichgans J. 2000. Glutathione, oxidative stress and neurodegeneration. Eur. J. Biochem. (267)4904-11.
Shanker G, Aschner M. 2003. Methylmercury-induced reactive oxygen species formation in neonatal cerebral astrocytic cultures is attenuated by antioxidants. Molecular Brain Research. (110):85-91.
Shulman RG, Rothman DL, Behar KL, Hyder F. 2004. Energetic basis of brain activity: implications for neuroimaging. Trends Neurosci. 27(8):489-95.
Skullerud K, Marstein S,Schrader H,Brunde let PJ, Jellum E. 1980. The cerebral lesions in a patient with generalized glutathione deficiency and pyroglutamic aciduria (5-oxoprolinuria). Acta Neuropathol (52):235-238.
Sorensen N, Murata K, Butz-Jorgensen E, Weihe P, Grandjean P. 1999. Prenatal methylmercury exposure as a cardiovascular risk factor at seven years of age. Epidemiology. 10(4):370-5.
Stajich GV, Lopez GP, Harry SW, Sexson WR. 2000. Iatrogenic exposure to mercury after hepatitis B vaccination in preterm infants. J Pediatr. 136(5):679-81.
Stohs SJ, Bagchi D. 1995. Oxidative mechanisms in the toxicity of metal ions. Free Radical Biology & Medicine. 18(2)321-336.
Tandon SK, Singh S, Prasad S, Khandekar K, Dwivedi VK, Chatterjee M, Mathur N. 2003. Reversal of cadmium induced oxidative stress by chelating agent, antioxidant or their combination in rat. Toxicol Lett. 10(145)3:211-7.
Ueha-Ishibashi T, Oyama Y, Nakao H, Umebayashi C, Nishizaki Y, Tatsuishi T, Iwase K, Murao K, Seo H. 2004. Effect of thimerosal, a preservative in vaccines, on intracellular Ca(2+) concentration of rat cerebellar neurons. Toxicology. 195(1):77-84.
Vahter M, Berglund M, Akesson A, Liden C. 2002. Metals and Women's Health. Environmental Research Section A. (88):145-55.
Vargas D. 2004. Neuroglial activation and neuroinflammation in the brain of patients with autism. Annals of Neurology. DOI: 10.1002/ana.20315
Verstraeten T. 2004. Thimerosal, the Centers for Disease Control and Prevention, and GlaxoSmithKline. Pediatrics. 113(4):932.
Waly M, Olteanu H, Banerjee R, Choi SW, Mason JB, Parker BS, Sukumar S, Shim S, Sharma A, Benzecry JM, Power-Charnitsky VA, Deth RC. 2004. Activation of methionine synthase by insulin-like growth factor-1 and dopamine: a target for neurodevelopmental toxins and thimerosal. Mol Psychiatry 9(4):358-70.
Warkany J. 1966. Acrodynia - postmortem of a disease. Am J Dis Child (112):147-156.
Weiss B, Clarkson TW, Simon W. 2002. Silent latency periods in methylmercury poisoning and in neurodegenerative disease. Environ Health Perspect. 110(Suppl 5):851-4.
Westphal GA, Schnuch A, Schulz TG, Reich K, Aberer W, Brasch J, Koch P, Wessbecher R, Szliska C, Bauer A, Hallier E. 2000. Homozygous gene deletions of the glutathione S-transferases M1 and T1 are associated with thimerosal sensitization. Int Arch Occup Environ Health. 73(6):384-8.
White JF. 2003. Intestinal Pathophysiology in Autism. Society for Experimental Biology and Medicine. 228(6):639-49.
Wu MM, Chiou HY, Wang TW, Hsueh YM, Wang IH, Chen CJ, Lee TC. 2001. Association of blood arsenic levels with increased reactive oxidants and decreased antioxidant capacity in a human population of northeastern Taiwan. Environ Health Perspect. 109(10):1011-7.
Hidden Asthma Triggers
Research reveals two common culprits
by Teri Walsh
http://msn.prevention.com/article/0,5778,s2-1-77-18-353-1,00.html
A common pain reliever--or a glass of wine--could bring on an asthma attack, two studies suggest.
The first study looked at the effect of acetaminophen on 1,574 people, 664 of whom had asthma. (Acetaminophen is an active ingredient contained in Tylenol and other non-aspirin pain relievers.) Researchers found that the more acetaminophen that people with asthma took, the more often they woke up at night with symptoms and the worse their reported quality of life (Thorax, Apr 2000).
The reason: Acetaminophen may deplete an essential antioxidant in the lungs called glutathione, says lead study author Seif Shaheen, MD, PhD, researcher and senior lecturer at Guy's, King's and St. Thomas' School of Medicine, King's College, London.
The second study examined the effect of food and drink on 336 asthmatics. Researchers found that one-third believed that alcohol--especially red or white wine--made symptoms worse (The Jour. of Allergy and Clinical Immunology, Mar 2000). Evidence suggests that sulfite preservatives, histamines, or salicylates may be responsible, rather than the alcohol itself, says lead study author Hassan Vally, research scientist at the Asthma and Allergy Research Institute, Inc., in Nedlands, Western Australia.
Tylenol decreases glutathion. Many of us (myself included) foolishly gave our kids Tylenol after (and sometimes even before) vaccinating at the direction of our pediatricians to minimize the negative side effects of the vaccines (like fever, crankiness, etc). My oldest son was vaccinated through age 2 and had tylenol OFTEN after vaccines as well as all of the times he was sick (which was almost constantly following his MMR). His lab results showed that he had virtually NO glutathion. My youngest was vaccinated through age 5 mos and almost never had tylenol (maybe 2x in his whole life through age 4) and his glutathion levels were very good. Just
one more reason I could kick myself for the rest of my life. No time, got to move on, think positive and heal my kids. Below is info on the importance of glutathion from TACA's website:
Glutathione helps to defend the body against damage from cigarette smoking, exposure to radiation, cancer chemotherapy, and toxins such as alcohol. As a detoxifier of heavy metals and drugs, it aids in the treatment of blood and liver disorders. Glutathione protects cells in several ways. It neutralizes oxygen molecules
before they can harm cells. Together with selenium, it forms the enzyme glutathione peroxidase, which neutralizes hydrogen peroxide. It is also a component of another antioxidant enzyme, glutathione-S-transferase, which is a broad-spectrum liver-detoxifying enzyme.
Glutathione protects not only individual cells but also the tissues of the arteries, brain, heart, immune cells, kidneys, lenses of the eyes, liver, lungs, and skin against oxidant damage. It plays a role in preventing cancer, especially liver cancer, and may also have an anti-aging effect. Glutathione can be taken in supplement form. The production of glutathione by the body can be boosted by taking supplemental N-acetylcysteine or L-cysteine plus L-methionine. Studies suggest that this may be a better way or raising glutathione levels than taking glutathione itself. Glutathione is not technically an amino acid, however, due to its close relationship is normally grouped with the amino acids. Most glutathione is found in the liver where it detoxifies many harmful compounds to be excreted thru the bile. Some glutathione is released directly by the liver into the bloodstream where it helps to maintain the strength of your red blood cells and also protecting your white blood cells.
Glutathione can also be found in the lungs and in your body's intestinal tract system. It is required for carbohydrate metabolism. Glutathione also appears to have anti-aging effects by aiding in the breakdown of oxidized fats that may contribute to atherosclerosis. As we get older glutathione levels in the body get lower and this can cause an increase in the aging process. Thus glutathione supplementation is useful to prevent this from occurring. Glutathione deficiency maybe indicated by: coordination problems, mental disorder, tremors, twitching, nervous system disorder, and difficulty in balancing. Currently, believed to be caused by lesions in the brain.
Severity of Autism Is Associated With Toxic Metal Body Burden and Red Blood Cell Glutathione Levels
Adams J et al
Journal of Toxicology
Provisional PDF:
http://www.hindawi.com/journals/jt/aip.532640.pdf
Abstract: This study investigated the relationship of children’s autism symptoms with their toxic metal body burden and red blood cell (RBC) glutathione levels. In children ages 3-8 years, the severity of autism was assessed using four tools: ADOS, PDD-BI, ATEC, and SAS. Toxic metal body burden was assessed by measuring urinary excretion of toxic metals, both before and after oral dimercaptosuccinic acid (DMSA). Multiple positive correlations were found between the severity of autism and the urinary excretion of toxic metals. Variations in the severity of autism measurements could be explained, in part, by regression analyses of urinary excretion of toxic metals before and after DMSA and the level of RBC glutathione (adjusted R2 of 0.22-0.45, p<0.005 in all cases). This study demonstrates a significant positive association between the severity of autism and the relative body burden of toxic metals.
