Excerpted From the House of Representatives Gov't Reform Committee Staff
Report
http://www.whale.to/v/staff.html
Application to the FDA
December 9, 1994
Fred Clark, Paul Offit, Stanley
Plotkin (Inventors); Wistar
Institute of Anatomy and
Biology and Children's Hospital
of Pennsylvania (Assignees)
Filed U.S. Patent for Rotavirus reassortant vaccine. Application number 353547
Dr. Offit shares the patent on the Rotavirus vaccine in development by Merck and lists a $350,000 grant from Merck for Rotavirus vaccine development. Also, he lists that he is a consultant to Merck.
c. Dr. Paul Offit
Dr. Offit lists that he is a consultant to Merck on an attachment to his OGE 450, but does not disclose whether or not he received any remuneration for his services.
(Exhibit 39)
Dr. Offit began his tenure on ACIP in October of 1998. Out of four votes pertaining to the ACIP’s rotavirus statement he voted “yes” three times, including, voting for the inclusion of the rotavirus vaccine in the VFC program.
Dr. Offit abstained from voting on the ACIP’s rescission of the recommendation of the rotavirus vaccine for routine use. He stated at the meeting, “I’m not conflicted with Wyeth, but because I consult with Merck on the development of rotavirus vaccine, I would still prefer to abstain because it creates a perception of conflict.”[lxvii]
In the hearings in the House
He was questioned continually by Dan Burton, Congressman in the Conflict of Interest Hearings in D.C. about his conflicts and he ABSOLUTELY denied that the above made a conflict because he was an honest man.
http://nachrichten.boerse.de/anzeige.php3?id=775c11cf
Vaccine-Preventable Diseases Rotavirus vaccines on the horizon offer some hope Future vaccines may include bovine and attenuated human rotavirus strains.by Colleen Zacharyczuk
Managing Editor
June 2003
SEATTLE – Future rotavirus vaccines may include both bovine and attenuated human rotavirus strains. They are believed to be unlikely to induce intussusception, and should still be effective, according to Paul Offit, MD, who spoke here at the Pediatric Academic Societies meeting.
Offit, of the Children’s Hospital of Philadelphia, at the University of Pennsylvania School of Medicine, said there are two new rotavirus vaccines on the horizon that may make a dent in the tremendous disease burden caused by rotavirus.
In developing countries, rotavirus is a deadly disease, accounting for approximately 660,000 to 800,000 deaths a year from severe dehydration. It is because of the disease burden that a vaccine is needed, Offit said.
Initially, the first rotavirus vaccine, the live, oral tetravalent RotaShield (RRV-TV, Wyeth-Ayerst) vaccine was developed using a simian rotavirus.
The approval of RotaShield in 1998 was based on positive evaluation of efficacy data from five, large clinical efficacy trials conducted in the United States and Europe. Offit said that the vaccine was about 48% to 68% protective against disease. There were some adverse events, including fever, decreased appetite, irritability and decreased activity after the first dose — these events were not observed after the second dose.
Another problem noted before the vaccine was licensed was intussusception. It was noted in five of 10,992 vaccine recipients, and one per 4,633 placebo recipients. According to Offit, this fact was worrisome enough to be included in the package insert.
About one year after the vaccine was licensed, a Morbidity and Mortality Weekly Report noted 15 cases of intussusception, 13 of which had occurred after the first dose and 11 of which had occurred within seven days of the vaccine’s administration.
The CDC suspended use of the vaccine while a case study was performed, and after that study, researchers determined that the relative risk was highest after the first dose, and declined after the second dose. The risk for intussusception was about one case per 10,000 vaccine recipients. Because of the risk of intussusception, the vaccine’s manufacturer pulled the vaccine from shelves and health officials suspended its use.
During the time that RRV-TV was available, approximately 1 million American infants were immunized, and one child died of vaccine-related intussusception. “One could argue the benefits of the vaccine still outweighed its risk,” Offit said. “There would be far fewer hospitalizations and deaths from intussusception than from rotavirus disease.”
Vaccines in the pipeline
The fact that the vaccine has been pulled from shelves left other companies looking for alternative vaccine strategies. So far, most candidate vaccines against rotavirus have been based on live, weakened animal strains of the virus. These animal strains were used at first, in part, because they grew easily in cell cultures. RRV-TV is based on a strain from the rhesus macaque, but Merck has a candidate based on a bovine strain known as WC3 (RotaTeq).
In developing countries, rotavirus is a deadly disease, accounting for approximately 660,000 to 800,000 deaths a year from severe dehydration.
The WC3 vaccine is a liquid, buffered vaccine that has been administered orally on the two-, four-, six-month and two-, three-, four-month schedule in clinical trials. It is a multivalent vaccine with specificity against the four serotypes — G1, G2, G3 and G4, that are responsible for more than 85% of rotavirus gastroenteritis worldwide.
In several placebo-controlled studies done to date, WC3 and its parent vaccines have been generally well tolerated and efficacious. No statistically significant increase in the incidences of fever, irritability, vomiting, or diarrhea has been observed in vaccine as compared with placebo recipients. For example, in a study of 439 infants, 15.7% of vaccine recipients vs. 14.1% of placebo recipients had fever during the two-week period after dose 1. The proportion of patients who shed vaccine in stools is low, ranging from 3.3% to 4.4% during the three to five days after vaccination.
Offit said a completed study of 1,946 infants who were followed for gastroenteritis throughout the rotavirus season after vaccination, suggests that RotaTeq was 68.8% to 76.6% efficacious in preventing any rotavirus disease regardless of severity or serotype. Preliminary immunogenicity results show a three-fold rise in serum neutralizing antibody titer to G1 in 73.3% to 86.2% of vaccinees, and a three-fold rise in rotavirus-specific serum IgA in >90% of vaccinees.
A large study is underway to evaluate the safety of the vaccine with respect to serious adverse experiences such as intussusception. He said no evidence of intussusception associated with the new vaccine has been noted, yet, in 45,000 infants in clinical trials.
Another option for a rotavirus vaccine lies with the attenuated human rotavirus vaccine (RotaRix, GlaxoSmithKline). Offit said this a phase-2 efficacy study of 215 infants had positive results, with approximately 90% of the vaccinated infants protected from rotavirus and a statistical significance at P<0.001. Examination of the safety data revealed only mild transient symptoms including fever in a small number of infants.
For more information:
Offit P. New rotavirus vaccines: after Rotashield. Topic symposium 5654. Presented at the Pediatric Academic Societies meeting. May 3-6, 2003. Seattle.
Dr. Offit is a coholder of the patent on bovine-human reassortant rotavirus vaccine currently being developed by Merck.
Safety, efficacy, and immunogenicity of a live, quadrivalent human-bovine reassortant rotavirus vaccine in healthy infants.
Clark HF, Bernstein DI, Dennehy PH, Offit P, Pichichero M, Treanor J, Ward RL, Krah DL, Shaw A, Dallas MJ, Laura D, Eiden JJ, Ivanoff N, Kaplan KM, Heaton P.
University of Pennsylvania School of Medicine, Philadelphia, and Merck & Co, Inc, West Point, Pennsylvania USA.
OBJECTIVES: To investigate safety, efficacy, and immunogenicity of live quadrivalent rotavirus vaccine (QRV) containing human-bovine (WC3) reassortant rotavirus serotypes G1, G2, G3, and P1a.Study design This was a randomized, double-blinded, placebo-controlled trial. During 1993 to 1994, at 10 US study sites, 439 healthy infants approximately 2 to 6 months of age, were enrolled to receive 3 doses of oral QRV or placebo at approximately 8-week intervals.
RESULTS: The vaccine was generally well tolerated; no serious vaccine-related adverse experiences were reported. Risk differences and 95% confidence intervals suggested no differences between vaccine and placebo recipients in the incidences of fever, irritability, vomiting, or diarrhea during the 14 days after any dose. QRV was 74.6% efficacious (95% CI: 49.5%, 88.3%) in preventing rotavirus acute gastroenteritis (AGE), regardless of severity and 100% efficacious (95% CI: 43.5%, 100%) in preventing severe rotavirus AGE through one rotavirus season. Serotype G1 was identified in most infants with rotavirus AGE. A >/=3-fold rise in serum neutralizing antibody to G1 was observed in 57% (45/79) of vaccinees. A >/=3-fold rise in serum anti-rotavirus IgA and fecal anti-rotavirus IgA was observed in 88% (162/185) and 65% (104/159) of vaccinees, respectively. CONCLUSIONS: QRV was generally well tolerated, immungenic, and highly effective against rotavirus gastroenteritis.
PMID: 14760258 [PubMed - in process]
VACCINE EXPERT OFFIT DODGES VACCINE-MERCURY DEBATE ON MSNBC, SAYS
NATIONAL AUTISM ASSOCIATION
http://www.nationalautismassociation.org/press062405.php
PRESS RELEASE
For Immediate Release:
June 24, 2005
Contact:
Laura Bono, NAA (NC) 919-403-9443
Jo Pike, NAA (SC) 843-206-8443
Rita Shreffler, NAA (MO) 417-725-6107
Wendy Fournier, NAA (RI) 401-632-7523
VACCINE EXPERT OFFIT DODGES VACCINE-MERCURY DEBATE ON MSNBC, SAYS NATIONAL AUTISM ASSOCIATION
DR. PAUL OFFIT AND OTHER EXPERTS AGAIN DECLINE DEBATE ON THIMEROSAL ISSUE
New York, NY - Yesterday on MSNBC's Connection: Coast-to-Coast, Dr. Paul Offit, Chief of Infectious Diseases at the Children's Hospital of Philadelphia, declined to argue his case that mercury in vaccines is safe. The one-hour segment featured Offit, along with Dr. Louis Cooper, former President of the AAP. Both requested not to debate journalist David Kirby, whose best-selling book Evidence of Harm demonstrates a growing body of evidence that mercury in vaccines and other products cause autism.
Many wonder why pro-mercury experts, who tout thimerosal's safety, continue to shy away from healthy questioning. Richard Copeland (Springfield, OH) grandparent of a child with autism says, "This is how people act when they have something to hide."
More from Dr. Offit and Dr. Cooper:
- Offit contradicted his earlier public statements that the rise in autism is real, citing the criteria for autism may have simply been "loosened." Multiple studies conducted by UC Davis and Pediatrics conclude the rise is real.
- At a 2004 meeting in Chapel Hill, NC, Offit suggested that something must be happening during pregnancy to cause autism, yet thimerosal is a post-natal toxin. A mother pointed out that thimerosal is also given pre-natally via immunoglobulins such as RhoGAM. Offit replied, "[Thimerosal] shouldn't have been in there."
- On MSNBC, Offit made reference to Swine-flu vaccines causing Guillain-Barre, an autoimmune disorder. In Chapel Hill, Offit claimed that "no vaccine has ever caused an autoimmune disorder." Many feel autism is autoimmune related.
- On MSNBC, Offit discussed the "massive inadvertent mercury poisoning" in Iraq in the early 70's, stating that pregnant Iraqi mothers who ate mercury-laden food had babies with mental retardation and seizure disorders, not autism. However, mental retardation and seizure disorders are sub-symptoms of autism, as well as hearing problems, digestive problems, kidney issues and other symptoms associated with the Iraqi poisoning.
- Offit claimed it is "very simple" to do retrospective epidemiological studies; however, the CDC had to do their epidemiological study five times, one of which found a connection but was never released.
- Offit said the epidemiological studies were "carefully performed." Yet, in 2004 National Journal quoted Dr. Robert Davis admitting they allowed newborn babies into the inclusion criteria, even though newborns are too young to be diagnosed with autism.
- Offit said that mercury (a neurotoxin) causing autism (a neurodevelopmental disorder) does not make biological sense. Yet, in October 2001, the IOM concluded that it was "biologically plausible."
- Dr. Cooper suggested the simultaneous increase between the rise in autism, now affecting 1 in 166 children, and vaccine-based thimerosal, is a mere "coincidence." Many feel that autism, which was first diagnosed right around the same time thimerosal was introduced, is also a coincidence. Further, pro-mercury advocates feel that parental reports of their children's immediate regression following a thimerosal-based vaccine, is also a coincidence.
Offit championed epidemiological studies which mainly work off numbers and statistics. Earlier in the segment, Kirby pointed out that major universities have performed peer-reviewed biological studies, a more powerful indicator of causation. These studies suggest mercury-based thimerosal causes autistic-like behaviors. The behavioral and medical symptoms of autism and mercury poisoning are virtually identical. To view these studies, please visit www.nationalautism.org
Think Autism. Think Cure.
National Autism Association | PO Box 1547 | Marion | SC | 29571
A vaccine for rotavirus (Rotateq) developed by Merck, the Children's Hospital of Philadelphia and Paul Offit, America's most quoted promoter and apologist for the vaccine industry, will be considered for licensure on December 14 and by the Vaccines and Related Biological Products Advisory Committee of the Center for Biologics Evaluation and Research of the FDA.
Offit and his partners Merck and the Chidren's Hospital of Philadelphia, first received a patent for a rotavirus vaccine in 1994. Offit later voted to add rotavirus vaccine (a variety from Wyeth not Merck) to the recommended schedule of vaccines when he was a member of the FDA's Advisory Committee of Immunization Practices. Despite his ownership of a rotavirus vaccine patent Offit saw no need to recuse himself from several votes on adding rotavirus to the schedule, which is one of the last steps to inclusion in the mandatory schedules, and a guaranteed market worth billions to a vaccine maker, and comes with complete immunity from lawsuits.
This vaccine was rushed into distribution has quickly shown to cause massive intestinal damage and death in a small but vulnerable subset of children. It was just as quickly removed form the market.
According to the FDA website three of the members of the Committee's members have applied for and received waivers for potential conflicts of interest
Participation of the public is permitted in this meeting:
December 14 - 15, 2005 Meeting
Date and Time:
The meeting will be held on December 14, 2005, 9:00 am to 4:30 pm; and on December 15, 2005, 9:00 am to 4:30 pm
Location:
Holiday Inn Select, 8120 Wisconsin Avenue, Bethesda, MD, 20814, 301-652-2000 .
Contact Persons:
Christine Walsh, R.N. or Denise Royster, 301-827-0314, or FDA Advisory Committee Information Line, 1-800-741-8138 (301-443-0572 in the Washington, DC area), code 3014512391. Please call the Information Line for up-to-date information on this meeting.
Agenda:
On December 14, 2005, the Committee will hear presentations and make recommendations on the safety and efficacy of a Rotavirus Vaccine manufactured by Merck. On December 15, 2005, the Committee will hear presentations and make recommendations on the safety and efficacy of ZOSTAVAX (Zoster Vaccine Live [Oka/Merck] ) manufactured by Merck.
Oral Presentations:
Between approximately 1:15 and 1:45 pm, on December 14, 2005; and 1:30 and 2:00 pm on December 15, 2005, oral presentations from the public will be scheduled. Those desiring to make formal oral presentations should notify the contact person before December 7, 2005.
RotaTeq®
Paul Offit at The Children's Hospital of Philadelphia developed a vaccine based on a bovine strain of rotavirus (WC-3). Merck is currently running Phase III trials of a modified version of his quadravalent reassortant vaccine. Aiming to avoid the adverse affects that RotaShield® was associated with, the vaccine is based on a bovine strain of rotavirus. The bovine strain was chosen because it replicates less prolifically in the human gastrointestinal tract than the simian strain used for the tetravalent rhesus reassortant vaccine. [1] Each of the five reassortants consists of the genetic backbone of the bovine virus with an inserted gene coding for a different human rotavirus surface protein. The inserted genes were selected to represent a broad range of serotypes in order to elicit protection against a wide variety of strains.
Genes coding for four VP7 proteins and one VP4 protein are included in the reassortants. Human serotypes G1, G2, G3 and G4 are represented by the four VP7 proteins, and serotype P1a is represented by the VP4 protein. [2] Initial trials of a similar live quadrivalent human-bovine reassortant vaccine demonstrated promising protection against rotavirus infection. [3] Differing from the Merck vaccine only by the exclusion of serotype G4, this vaccine's results likely mirror the protection that RotaTeq® will afford.
The quadrivalent vaccine, which was delivered to vaccinees in three oral doses at 2, 4, and 6 months of age (identical to the Merck vaccine delivery schedule), showed 74.6% efficacy against any rotavirus infection and 100% efficacy against severe rotavirus infection. No increase in diarrhea, vomiting, fever or irritability was reported as compared to the recipients of the placebo. The immunogenicity of the quadrivalent vaccine was reflected in an increased ratio of rotavirus specific IgA to total IgA as measured in the vaccinee's stool. [3] Licensure of RotaTeq® by the FDA is predicted for 2005 if Phase III trials are successful.
MEDIA
The Cutter Incident: How America's First Polio Vaccine Led to the Growing
Vaccine Crisis -- by M.D., Paul A. Offit
Book Reviewed by John Gilmore
This is a truly bizarre book. Somehow the author Paul Offit, MD, believes that telling a gripping story about the massive scientific, regulatory and industrial failures that lead to hundreds of thousands of people in 1955 being injected with a vaccine containing live polio viruses which resulted in thousands of people paralyzed for life and hundreds of deaths, would persuade people now that vaccine manufacturers should be shielded from any legal liability for their products. That in a nutshell is the purpose of this book.
The first 130 pages tells the compelling story of the development of the polio vaccine and how a batch of polio vaccine made by Cutter Laboratories actually gave people the disease it was designed to prevent. This section is followed by a forty-page analysis of the legal consequences of the Cutter incident that verges on incoherence. Here Offit seems to make the classic mistake of physicians who assume they are the leading authority in the room on all subjects. Somehow Offit believes that a fundamental injustice to the vaccine industry occurred when juries found that Cutter Laboratories was liable for the damage created by their product. In Offit’s analysis, as long as the pharmaceutical company thought the vaccine was safe, injured people should have no legal recourse. It would seem obvious that shielding firms from liability creates exactly the kind of environment where Cutter-type incidents would breed.
This section is followed by a brief polemic, more of a rant, filled with factual errors, demanding the laundry list of political favors lusted after by the pharmaceutical industry. These demands go far beyond “tort reform,” the pharmaceutical industry is calling for the repeal of basic constitutional rights and the undermining of basic principles of American
law to suit the short-term profit needs of a generously campaign-donating industry.
While stating his academic and hospital associations, the book fails to disclose significant and relevant details of Offit's own financial and business dealings. In addition to being the leading vaccine promoter in the US, just google him, he is also a vaccine developer and business partner with Merck, GlaxoSmithKline and the Children’s Hospital of Philadelphia, who collectively own a rotavirus vaccine that was recently overcame a major milestone to licensure.
+ Continues here: http://www.sarnet.org/lib/SARrev1-16-06.htm
The debate over whether or not vaccines contribute to the onset of autism is heating up. I commented on another vaccine-autism article just a few days ago. If you missed it, please review it now to find out more about common sense prevention strategies, and how you can treat autism if your child has it.
But today, I’d like to talk about misinformation, deception, and personal agendas.
Who is Dr. Paul Offit?
Some of you may recognize the name of Dr. Paul Offit, as he is a fairly frequent commentator for the pro-vaccination camp. But what do you know about Dr. Offit?
Dr. Offit, a.k.a. Paul “For Profit” Offit, by some vaccination opponents, is not just a doctor who believes that vaccinations save lives.
Dr. Offit is also one of the patent holders of the rotavirus vaccine (Patent Application number 353547), and the recipient of a $350,000 grant from Merck for its development. Additionally, he is a consultant to Merck Pharmaceuticals.
Talk about conflict of interest. Jeesh! But that's not all.
The Advisory Committee on Immunization Practices (ACIP) is a 15 member panel of immunization experts, selected by the Secretary of the U. S. Department of Health and Human Services. They provide advice and guidelines to the Secretary for Health the Centers for Disease Control and Prevention (CDC) on vaccine-preventable diseases.
As a member of the ACIP, starting in 1998, Dr. Offit voted “yes” three times out of four on issues pertaining to the ACIP’s rotavirus statement, including, voting for his own vaccine to be included in the immunization schedule.
He is also the doctor whose incomprehensible statement, “an infant can safely receive up to 10,000 vaccines at once,” will live on in infamy.
So the question is: if YOU held a patent for a product of enormous income potential, would you even consider the possibility that your cash-cow might be doing more harm than good? Would you admit that a similar product might be the cause of needless suffering?
And if you WERE able to consider it, would you admit there might indeed be a problem?
Here’s the deal, folks. It’s not enough to look at the obvious credentials of your spokesmen, whether they’re pro- or anti- an issue. Today, you also have to consider the hidden motivations behind their recommendations. Where is their loyalty? How do they feed themselves? And by that I don’t mean, “what’s their nutritional type?” I mean, who pays for their lifestyle? Where is the money coming from?
Do you believe Dr. Offit is an independent, neutral expert on the vaccination issue? Do you believe he’s looked at both sides and made an educated and honest judgment call?
I guess that depends on just how independent and honest you believe a man can be when there’s pharmaceutical patent money at stake.
Hilleman’s Confidential Memo
To give you another glimpse of the reality behind the Big Pharma curtain, Maurice R. Hilleman, Ph.D. is another leading expert on immunization, in the sense that he developed more than 40 vaccines and published close to 500 articles on virology, infectious diseases, epidemiology and immunology.
In 2005, a confidential memo was discovered that was written in 1991 by then senior Merck Vice-President, Maurice Hilleman, to Dr. Gordon Douglas, then head of Merck's vaccine division. (Douglas is now a consultant for the Vaccine Research Center at the National Institutes of Health.)
In the memo, Dr. Hilleman wrote:
“The regulatory control agencies in some countries, particularly Scandinavia (especially Sweden) but also UK, Japan, and Switzerland have expressed concern for thimerosal, a mercury preservative, in vaccines. Some countries require absence of thimerosal from single-dose package. This trend will probably spread… Sweden is requiring thimerosal free single-dose packaging of all products as soon as can be reasonably achieved. The deadline for DT is January, 1992… “
The focal point for present concern is in Scandinavia… The immediate Merck concern is to be able to qualify for sale of single-dose products in Sweden and in Norway and Denmark…
The public awareness has been raised by the sequential wave of experiences in Sweden including mercury exposure from additives, fish, contaminated air, bird death from eating mercury-treated seed grains, dental amalgam leakage, mercury allergy, etc… In some instances, public immunization programs may be endangered by public refusal to accept vaccines with thimerosal.”
Dr. Hilleman went on:
“For babies: The 25 µg of mercury in a single 0.5 ml dose and extrapolated to a 6 lb baby would be 25X the adjusted Swedish daily allowance of 1.0 µg for a baby of that size…
If 8 doses of thimerosal-containing vaccine were given in the first 6 months of life (3 DPT, 2 HIB and 3 Hepatitis B) the 200 µg of mercury given, say an average size of 12 lbs would beabout 87X the Swedish daily allowance of 2.3 µg of mercury for a baby of that size.”
And finished off the memo with the statement:
"The U.S. Food and Drug Administration ... does not have this concern for thimerosal."
So, in 1991, the premier U.S. vaccine expert told the chief of the largest U.S. vaccine manufacturer that they had to immediately produce mercury-free vaccines for Scandinavian children because the Scandinavians refused to expose their children to these unacceptable levels of mercury, which would eliminate Merck’s Scandinavian market share.
(It should also be noted that the Swedish maximum daily allowance of mercury from fish is roughly the same guideline used by the U.S. FDA.)
Meanwhile, the U.S. continued to produce and administer mercury-containing vaccines to American children throughout the 90’s. It wasn’t until 1999 that U.S. federal health officials admitted that infants were in fact being exposed to mercury through their vaccinations.
Are ALL Vaccines Now Mercury-Free?
NO! They’re NOT!
That’s another cry you hear over and over again: that “we’ve now removed mercury from all vaccines.”
But a more accurate statement would be that mercury has been removed from MOST vaccines – not all – and several still contain traces of mercury, at a level so low the actual amount doesn’t have to be stated.
Here is the most current schedule (updated January 28, 2008) disclosing the amount of thimerosal and mercury contained in U.S. vaccines. It’s also available as a printable PDF.
The following vaccines still contain 25 mcg of mercury per 0.5 ml:
DTwP
DT (diphtheria and tetanus) multi-dose vial
Tetanus
Several brands of the 2006/2007 influenza formulas
Meningococcal multi-dose vial
Interestingly, as they’ve removed mercury from most childhood vaccinations, the flu shots still have plenty of it – courtesy of a 2007 Presidential veto against its removal. And guess what? Now the standard recommendation is to vaccinate your child against the flu EVERY YEAR. Come on!
Why the persistent insistence on injecting mercury into our children?
How Much Does Conventional Medicine Know?
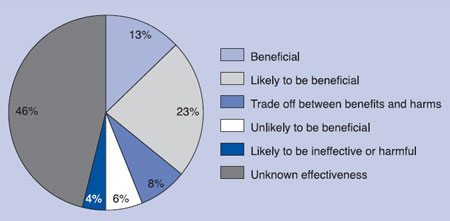
That’s actually a great question, and it was originally posed, not by me, but by the journal BMJ Clinical Evidence.
They found that of about 2,500 treatments offered in conventional medicine:
13 percent are beneficial to the patient
23 percent are likely to be beneficial
8 percent is a trade-off between benefits and harm
6 percent are unlikely to be beneficial
4 percent are likely to be ineffective or harmful
46 percent have unknown effectiveness