
See more at: http://www.vaccinationcouncil.org/2012/03/09/common-vaccine-ingredient-implicated-in-nejm-article-as-causative-in-serious-type-of-kidney-disease-by-suzanne-humphries-md/#sthash.u2gPcVlh.dpuf
Common vaccine ingredient implicated in NEJM article as causative in serious type of kidney disease. By Suzanne Humphries, MD
March 9, 2012Posted in: Articles Print PDFA June, 2011 New England Journal Of Medicine article titled “Early-Childhood Membranous Nephropathy Due to Cationic Bovine Serum Albumin”
[1] recently caught my attention. Namely, because it admits the plausible association between circulating cationic bovine(cow) serum albumin (BSA, a common vaccine ingredient) and a very difficult-to-treat form of kidney disease called idiopathic membranous nephropathy (IMN). Skeptics often demand peer-reviewed articles to support the fact that vaccines cause bodily harm. Often, while we know what we see in front of us, “scientific” proof is non-existent due to lack of motivation by researchers in exploring the likely associations.
Well, here in one of the world’s most respected medical journals lies some very interesting information, and it was conducted by two renowned nephrologists. Dr. Giuseppe Remuzzi is an expert in the field of protein trafficking within the kidney, and Dr. Pierre Ronco is a well-known and highly respected nephrologist.
First, let me explain what nephrotic syndrome and membranous nephropathy are. Nephrotic syndrome is a condition where the kidneys leak large amounts of protein into the urine and is defined in detail HERE. The term just describes a clinical condition that can have one of several causes. This article discusses one cause called membranous nephropathy.
The kidney is composed of millions of microscopic filters that cleanse the blood. This is a schematic of one of those filters.
- See more at: http://www.vaccinationcouncil.org/2012/03/09/common-vaccine-ingredient-implicated-in-nejm-article-as-causative-in-serious-type-of-kidney-disease-by-suzanne-humphries-md/#sthash.u2gPcVlh.dpuf
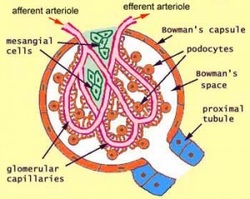
Approximately one quarter of the blood leaving the heart goes to the kidneys, which filter 140- 180 liters of your blood per day. In health, the kidneys retain your albumin and proteins and filter excess water, toxins and minerals. The filters are composed of membranes that are negatively charged and thus repel negatively charged molecules like your own proteins.
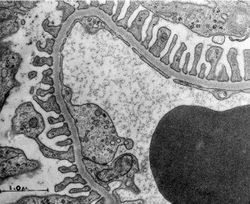
Here is an electron microscope photo of a normal glomerular capillary membrane, the thing that serves as a filter for your blood. It is a close-up photo of the schematic from above.
Here is an electron microscope photo of a normal glomerular capillary membrane, the thing that serves as a filter for your blood. It is a close-up photo of the schematic from above.
Below is a similar photo of a membrane that contains deposits of antibody attached to bovine serum albumin trapped in the membrane – as in membranous nephropathy.(MN)
- See more at: http://www.vaccinationcouncil.org/2012/03/09/common-vaccine-ingredient-implicated-in-nejm-article-as-causative-in-serious-type-of-kidney-disease-by-suzanne-humphries-md/#sthash.u2gPcVlh.dpuf
- See more at: http://www.vaccinationcouncil.org/2012/03/09/common-vaccine-ingredient-implicated-in-nejm-article-as-causative-in-serious-type-of-kidney-disease-by-suzanne-humphries-md/#sthash.u2gPcVlh.dpuf
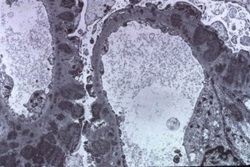
It should now be obvious why this creates dysfunction and leakage of the filter.
Because the cationic bovine serum albumin carries a positive charge, it will be more difficult for the membrane to effectively impede the protein during the filtration process. And…when the bovine serum albumin is attached to an antibody, the complex may deposit in the membrane of the kidney. This leads to inflammation and breakdown of the filter membrane barrier, allowing it to leak important bodily proteins, clotting factors, immune globulins etc. that normally would be held back in the selective filtration process. Some diseases that are “nephrotic” include idiopathic membranous nephropathy(IMN), minimal change nephropathy (MCN, most common in children), and focal and segmental glomerulosclerosis(FSGS,second most common in children). Protein-losing nephropathies like this result in several other problems in the body, namely high blood pressure, high cholesterol and kidney insufficiency. They can also lead to clotting disorders from loss of antithrombin, infections due to loss of important immune globulins, and vitamin D deficiency due to loss of vitamin D binding proteins among other things.
While the medical literature considers prognosis for IMN to be relatively good in adults, nephrologists are well aware that one-third of such cases progress to dialysis despite aggressive treatment. Doctors are aware of the potentially devastating side effects of treatment, which consists of very high doses of corticosteroids and immune-suppressing drugs such as cyclophosphamide or chlorambucil, prescribed for months. It is safe to say that once these drugs are used, the patient will never be the same, barring a miracle or aggressive alternative and nutritional/detoxification intervention. Atherosclerosis, cancer, and diabetes are among the more common side effects of these drugs. Life–threatening infections can and do occur.
Idiopathic membranous nephropathy (IMN) in children is a less-known entity and admittedly much more of a PROBLEM,
“IMN is a rare but serious glomerulopathy in pediatrics. Long-term prognosis is guarded because approximately 50% of patients may have evidence of progressive kidney disease.”[2]
While much of how we treat children is based upon experience in treating adults, treatment is not always parallel in success or side effects. Greater than 80% of membranous nephropathy in adults is IDIOPATHIC, and the best form of treatment is controversial. Treatment is always touch and go, and quite nerve racking to doctor and patient. Don’t you think that this degree of idiopathic disease is very high, given that idiopathic means that doctors will never determine the cause?
Idiopathic membranous nephropathy (IMN), the topic of the article, is more common among adults, and while relatively rare in children, may be on the rise. When children present with nephrotic syndrome, they are initially treated with a 28-day course of steroids. If they do not respond to that, they undergo a kidney biopsy. Nephrology literature suggests that the underlying pathology of childhood nephropathy is changing and has become more severe and steroid resistant.[3]
The NEJM article focuses on the 4 children and 11 adults of 50 membranous cases that had high levels of circulating anti–bovine serum albumin antibodies(anti-BSA). These patients also had elevated levels of circulating BSA. So, of all cases reviewed, 30% had pathological evidence that implicated a cow protein as causative, and none of them tested positive for milk allergy. As you continue reading, consider when and where infants might encounter BSA.
The article discusses how “patients with childhood membranous nephropathy have both circulating cationic bovine serum albumin and anti–bovine serum albumin antibodies. Bovine serum albumin is present in immune deposits, suggesting that cationic bovine serum albumin is pathogenic through binding to the anionic glomerular capillary wall and in situ formation of immune complexes, as shown in experimental models.”
Last year I wrote a rather long and fully-referenced TOME where I suggested that if doctors started to look for the cause of “idiopathic” kidney disease, they would discover readily identifiable stimuli, and among them will be vaccines. Here, the authors validate this suggestion:
“It is likely that a growing number of cases of “idiopathic” membranous nephropathy will be reclassified as secondary once nonglomerular antigens are identified.”
And while they implicate dietary cow’s milk as one possible stimulus, they ultimately squeeze in a little statement at the end, saying…
“Although further epidemiologic studies are needed, absorption of dietary modified bovine serum albumin and immunization against bovine serum albumin should be considered a potential cause of membranous nephropathy in young children and should prompt a search for bovine serum albumin in immune deposits.”
Why suggest a dietary source of BSA as causing “immunization,” when a key problem is that most vaccines have BSA in the manufacturing process and the end product? So are these children developing antibodies from the BSA in vaccines, or in milk? Which do you think sets a better situation for reactivity – ingestion or injection? Consider that SQUALENE and mineral oil have therapeutic effects when swallowed, but are quite inflammatory upon injection. Mineral oil was put in vaccines in the past and later removed for causing sterile abscesses and ulcerations. Squalene is developing a nasty reputation today when used as an adjuvant. Adjuvants such as aluminum and squalene are added to vaccines specifically to rev up the inflammatory response.
I find this discussion very interesting in view of what non-vaccinating doctors and parents favor – both breastfeeding and avoiding vaccinations. In the discussion of milk, the authors state:
“In young children, cow’s milk is a major source of bovine serum albumin.”
“IgG antibodies to cow’s milk proteins are present in virtually all infants exposed to cow’s milk and have been considered physiologic.”
“Anti–bovine serum albumin antibodies directed to other regions of bovine serum
albumin have been identified in rheumatoid arthritis and multiple sclerosis, where they cross react with collagen and myelin basic protein, respectively.”
Idiopathic membranous nephropathy has also been reported ELSEWHERE to be related to cow milk processing.
At this point you may be saying, “But they say these proteins are present in all infants exposed to cow’s milk and so how can you implicate cow’s milk?” It is because of what they say next, that we must consider cow’s milk together with vaccination as potentiating factors.
“Taken together, these observations suggest that at least two additional factors are necessary for membranous nephropathy to develop: the first is the physicochemical properties and amount of circulating antigen; the second is the predominance of the T-helper type 2 (Th2) immune response.”
The Th2 immune response is the one that the immune system gets thrown into after vaccination. This is common knowledge in immunology/vaccine literature.[4]
“Such reprogramming would, in concert with the Th2-polarizing effect of aluminium phosphate, dampen protective cellular immunity in general,” LINK HERE
and thought by the vaccinationists to be no problem at all.
Many studies have been done in experimental animals whereby membranous nephropathy is purposefully induced by injecting cationized bovine serum albumin intravenously.
“Membranous nephropathy developed only in the animals that were given chemically modified cationized bovine serum albumin intravenously after immunization with cationic bovine serum albumin.”…not by feeding it to them.
What that statement says, is that membranous nephropathy developed in the animals injected with bovine serum albumin; the same albumin that is in many vaccines.
“Membranous nephropathy is characterized by a predominant Th2 immune response”…the same immune response that vaccines elicit.
The authors must be aware that they hit upon a very touchy subject since they implicate “immunization” in the body of the article, but conclude by simply saying,
“If bovine serum albumin is detected [in kidney biopsy specimens], eliminating it from the diet could be beneficial.”
First off, it seems a bit late to eliminate bovine albumin from the diet of children after they’ve developed a devastating kidney disease, doesn’t it? If you take this NEJM article at face value, it may support the belief that cow’s milk– especially pasteurized cow’s milk which is a whole different nutrient than raw cow’s milk – is not good food for humans and reinforces the fact that infants should breast feed whenever possible. Additionally, mothers should not accept the dogma that formula is just as good for their babies as breast milk and that weaned children need cow’s milk in order to be healthy. Calves need cow’s milk. If you have any doubt as to the benefit of human milk for human infants and toddlers, read “Breastfeeding, missing the bigger picture.”
What the NEJM authors don’t say is that eliminating direct injection of bovine serum albumin may be beneficial in preventing the susceptible child or adult from developing kidney disease. The following list of BSA-containing vaccines could possibly throw children or adults onto dialysis and/or a kidney transplant and will require immune suppressing drugs either way.
MMRV (ProQuad) – measles, mumps, rubella, chicken pox
MMR (MMR-II)
Hep A (vaqta)
Pneumococcal (Pneumovax) – pneumococcal pneumonia
Rabies (Rab vert) – rabies
Td (Decavac) – Tetanus, diptheria
Japanese Encephalitis (Ixiaro)
Tdap (Boostrix) – Tetanus, diptheria, pertussis
Varicella (Varivax) – chicken pox
Zoster (Zostavax) – shingles
DtaP-IPV/Hib (Pentacel)
DTaP-HepB-IPV (Pediarix) – listed as having “bovine protein”
So I will say it… in an age where “idiopathic” and devastating kidney diseases occur in children, you might want to consider the health of your children’s kidneys before vaccinating them. Given that glomerulonephritis is a relatively low-incidence disease, it will take a miracle to get a study large enough to detect the difference between vaccinated and unvaccinated children, and we know that isn’t going to happen any time soon. In the meantime, recommendations for childhood vaccinations may consider the poor outcome in your child as part-and-parcel for “the greater good” of society.
While researchers occasionally stumble upon vaccine ingredients and accidentally show causation in childhood kidney disease, the cause for the most common form of childhood nephrotic syndrome, minimal-change disease (prevalence 15 per 100K, affecting mostly children under 10 years), remains unknown. The US Department of Health and Human Services/NIH says
“The condition most commonly associated with childhood nephrotic syndrome is minimal change disease. Doctors do not know what causes it.”LINK HERE
Today we have shown you that a less-common form of nephrotic syndrome could be caused by a common vaccine ingredient – Bovine Serum Albumin. How much minimal change nephrotic syndrome is caused by vaccine ingredients? We don’t know. Doctors just give children steroids to suppress the symptoms, never knowing what the cause was, and seem all too comfortable in labeling it “idiopathic.”
For now, parents have to rely on their common sense and good judgment.
References
[1] Debiec, H. et al., 2011, Early Childhood Membranous Nephropathy Due to Cationic Bovine Serum Albumin,” NEJM. Jun 2;364(22):2101-10.
[2] Chen, A. et al., 2007, “Idiopathic membranous nephropathy in pediatric patients: presentation, response to therapy, and long-term outcome.” BMC Nephrology, 8:11
[3] Filler, G. et al., 2003, “Is there really an increase in non-minimal change nephrotic syndrome in children?”Am J Kidney Dis, Dec;42(6):1107-13.
[4] White OJ, et al.,2012. “A genomics-based approach to assessment of vaccine safety and immunogenicity in children.”Feb 27;30(10) PMID 22230586
_______________________________________________________________________________________________________________________________
About the author: Dr. Suzanne Humphries is a conventionally educated medical doctor who has taken the walk into, around, and out of the allopathic paradigm. She fully and successfully participated in the conventional system for 19 years, witnessing first-hand how that approach fails patients and creates new disease time and again. Prior to medical school, she earned a bachelor’s degree in physics from Rutgers University. After two years as the head technician in a research biochemistry lab, she went to medical school, graduating from Temple University School of Medicine in 1993. She then studied internal medicine in the Bronx, NY where she completed her 3-year medical residency. At this juncture, Dr Humphries became more aware of the failures of primary care medicine, observing that doctors are largely trained to prescribe drugs and hunt down disease. Despite this approach, the patients continued to get sicker, requiring more drugs and ultimately developing degenerative diseases. Not wanting involvement in the generation of chronically ill patients, she opted to work at the other end of the allopathic continuum and completed a fellowship in Nephrology. After 14 years of practicing allopathic kidney medicine, her perspective on the overall success of the allopathic paradigm has developed and matured. She views allopathic medicine as an overused system- that when implemented as first line treatment across-the-board for mild illnesses and symptoms, will mostly just drive chronic illnesses deeper and more seriously into the patient.
Dr. Humphries has re-dedicated her life as a doctor. She recently moved beyond mainstream medicine, and is utilizing nontoxic means to help restore health in those who seek her assistance. Homeopathy, nutrition, micronutrients, and detoxification are among the modalities she implements. Dr. Humphries is on the board of directors of the International Medical Council on Vaccination. She lives in Maine, USA.
- See more at: http://www.vaccinationcouncil.org/2012/03/09/common-vaccine-ingredient-implicated-in-nejm-article-as-causative-in-serious-type-of-kidney-disease-by-suzanne-humphries-md/#sthash.u2gPcVlh.dpuf
Because the cationic bovine serum albumin carries a positive charge, it will be more difficult for the membrane to effectively impede the protein during the filtration process. And…when the bovine serum albumin is attached to an antibody, the complex may deposit in the membrane of the kidney. This leads to inflammation and breakdown of the filter membrane barrier, allowing it to leak important bodily proteins, clotting factors, immune globulins etc. that normally would be held back in the selective filtration process. Some diseases that are “nephrotic” include idiopathic membranous nephropathy(IMN), minimal change nephropathy (MCN, most common in children), and focal and segmental glomerulosclerosis(FSGS,second most common in children). Protein-losing nephropathies like this result in several other problems in the body, namely high blood pressure, high cholesterol and kidney insufficiency. They can also lead to clotting disorders from loss of antithrombin, infections due to loss of important immune globulins, and vitamin D deficiency due to loss of vitamin D binding proteins among other things.
While the medical literature considers prognosis for IMN to be relatively good in adults, nephrologists are well aware that one-third of such cases progress to dialysis despite aggressive treatment. Doctors are aware of the potentially devastating side effects of treatment, which consists of very high doses of corticosteroids and immune-suppressing drugs such as cyclophosphamide or chlorambucil, prescribed for months. It is safe to say that once these drugs are used, the patient will never be the same, barring a miracle or aggressive alternative and nutritional/detoxification intervention. Atherosclerosis, cancer, and diabetes are among the more common side effects of these drugs. Life–threatening infections can and do occur.
Idiopathic membranous nephropathy (IMN) in children is a less-known entity and admittedly much more of a PROBLEM,
“IMN is a rare but serious glomerulopathy in pediatrics. Long-term prognosis is guarded because approximately 50% of patients may have evidence of progressive kidney disease.”[2]
While much of how we treat children is based upon experience in treating adults, treatment is not always parallel in success or side effects. Greater than 80% of membranous nephropathy in adults is IDIOPATHIC, and the best form of treatment is controversial. Treatment is always touch and go, and quite nerve racking to doctor and patient. Don’t you think that this degree of idiopathic disease is very high, given that idiopathic means that doctors will never determine the cause?
Idiopathic membranous nephropathy (IMN), the topic of the article, is more common among adults, and while relatively rare in children, may be on the rise. When children present with nephrotic syndrome, they are initially treated with a 28-day course of steroids. If they do not respond to that, they undergo a kidney biopsy. Nephrology literature suggests that the underlying pathology of childhood nephropathy is changing and has become more severe and steroid resistant.[3]
The NEJM article focuses on the 4 children and 11 adults of 50 membranous cases that had high levels of circulating anti–bovine serum albumin antibodies(anti-BSA). These patients also had elevated levels of circulating BSA. So, of all cases reviewed, 30% had pathological evidence that implicated a cow protein as causative, and none of them tested positive for milk allergy. As you continue reading, consider when and where infants might encounter BSA.
The article discusses how “patients with childhood membranous nephropathy have both circulating cationic bovine serum albumin and anti–bovine serum albumin antibodies. Bovine serum albumin is present in immune deposits, suggesting that cationic bovine serum albumin is pathogenic through binding to the anionic glomerular capillary wall and in situ formation of immune complexes, as shown in experimental models.”
Last year I wrote a rather long and fully-referenced TOME where I suggested that if doctors started to look for the cause of “idiopathic” kidney disease, they would discover readily identifiable stimuli, and among them will be vaccines. Here, the authors validate this suggestion:
“It is likely that a growing number of cases of “idiopathic” membranous nephropathy will be reclassified as secondary once nonglomerular antigens are identified.”
And while they implicate dietary cow’s milk as one possible stimulus, they ultimately squeeze in a little statement at the end, saying…
“Although further epidemiologic studies are needed, absorption of dietary modified bovine serum albumin and immunization against bovine serum albumin should be considered a potential cause of membranous nephropathy in young children and should prompt a search for bovine serum albumin in immune deposits.”
Why suggest a dietary source of BSA as causing “immunization,” when a key problem is that most vaccines have BSA in the manufacturing process and the end product? So are these children developing antibodies from the BSA in vaccines, or in milk? Which do you think sets a better situation for reactivity – ingestion or injection? Consider that SQUALENE and mineral oil have therapeutic effects when swallowed, but are quite inflammatory upon injection. Mineral oil was put in vaccines in the past and later removed for causing sterile abscesses and ulcerations. Squalene is developing a nasty reputation today when used as an adjuvant. Adjuvants such as aluminum and squalene are added to vaccines specifically to rev up the inflammatory response.
I find this discussion very interesting in view of what non-vaccinating doctors and parents favor – both breastfeeding and avoiding vaccinations. In the discussion of milk, the authors state:
“In young children, cow’s milk is a major source of bovine serum albumin.”
“IgG antibodies to cow’s milk proteins are present in virtually all infants exposed to cow’s milk and have been considered physiologic.”
“Anti–bovine serum albumin antibodies directed to other regions of bovine serum
albumin have been identified in rheumatoid arthritis and multiple sclerosis, where they cross react with collagen and myelin basic protein, respectively.”
Idiopathic membranous nephropathy has also been reported ELSEWHERE to be related to cow milk processing.
At this point you may be saying, “But they say these proteins are present in all infants exposed to cow’s milk and so how can you implicate cow’s milk?” It is because of what they say next, that we must consider cow’s milk together with vaccination as potentiating factors.
“Taken together, these observations suggest that at least two additional factors are necessary for membranous nephropathy to develop: the first is the physicochemical properties and amount of circulating antigen; the second is the predominance of the T-helper type 2 (Th2) immune response.”
The Th2 immune response is the one that the immune system gets thrown into after vaccination. This is common knowledge in immunology/vaccine literature.[4]
“Such reprogramming would, in concert with the Th2-polarizing effect of aluminium phosphate, dampen protective cellular immunity in general,” LINK HERE
and thought by the vaccinationists to be no problem at all.
Many studies have been done in experimental animals whereby membranous nephropathy is purposefully induced by injecting cationized bovine serum albumin intravenously.
“Membranous nephropathy developed only in the animals that were given chemically modified cationized bovine serum albumin intravenously after immunization with cationic bovine serum albumin.”…not by feeding it to them.
What that statement says, is that membranous nephropathy developed in the animals injected with bovine serum albumin; the same albumin that is in many vaccines.
“Membranous nephropathy is characterized by a predominant Th2 immune response”…the same immune response that vaccines elicit.
The authors must be aware that they hit upon a very touchy subject since they implicate “immunization” in the body of the article, but conclude by simply saying,
“If bovine serum albumin is detected [in kidney biopsy specimens], eliminating it from the diet could be beneficial.”
First off, it seems a bit late to eliminate bovine albumin from the diet of children after they’ve developed a devastating kidney disease, doesn’t it? If you take this NEJM article at face value, it may support the belief that cow’s milk– especially pasteurized cow’s milk which is a whole different nutrient than raw cow’s milk – is not good food for humans and reinforces the fact that infants should breast feed whenever possible. Additionally, mothers should not accept the dogma that formula is just as good for their babies as breast milk and that weaned children need cow’s milk in order to be healthy. Calves need cow’s milk. If you have any doubt as to the benefit of human milk for human infants and toddlers, read “Breastfeeding, missing the bigger picture.”
What the NEJM authors don’t say is that eliminating direct injection of bovine serum albumin may be beneficial in preventing the susceptible child or adult from developing kidney disease. The following list of BSA-containing vaccines could possibly throw children or adults onto dialysis and/or a kidney transplant and will require immune suppressing drugs either way.
MMRV (ProQuad) – measles, mumps, rubella, chicken pox
MMR (MMR-II)
Hep A (vaqta)
Pneumococcal (Pneumovax) – pneumococcal pneumonia
Rabies (Rab vert) – rabies
Td (Decavac) – Tetanus, diptheria
Japanese Encephalitis (Ixiaro)
Tdap (Boostrix) – Tetanus, diptheria, pertussis
Varicella (Varivax) – chicken pox
Zoster (Zostavax) – shingles
DtaP-IPV/Hib (Pentacel)
DTaP-HepB-IPV (Pediarix) – listed as having “bovine protein”
So I will say it… in an age where “idiopathic” and devastating kidney diseases occur in children, you might want to consider the health of your children’s kidneys before vaccinating them. Given that glomerulonephritis is a relatively low-incidence disease, it will take a miracle to get a study large enough to detect the difference between vaccinated and unvaccinated children, and we know that isn’t going to happen any time soon. In the meantime, recommendations for childhood vaccinations may consider the poor outcome in your child as part-and-parcel for “the greater good” of society.
While researchers occasionally stumble upon vaccine ingredients and accidentally show causation in childhood kidney disease, the cause for the most common form of childhood nephrotic syndrome, minimal-change disease (prevalence 15 per 100K, affecting mostly children under 10 years), remains unknown. The US Department of Health and Human Services/NIH says
“The condition most commonly associated with childhood nephrotic syndrome is minimal change disease. Doctors do not know what causes it.”LINK HERE
Today we have shown you that a less-common form of nephrotic syndrome could be caused by a common vaccine ingredient – Bovine Serum Albumin. How much minimal change nephrotic syndrome is caused by vaccine ingredients? We don’t know. Doctors just give children steroids to suppress the symptoms, never knowing what the cause was, and seem all too comfortable in labeling it “idiopathic.”
For now, parents have to rely on their common sense and good judgment.
References
[1] Debiec, H. et al., 2011, Early Childhood Membranous Nephropathy Due to Cationic Bovine Serum Albumin,” NEJM. Jun 2;364(22):2101-10.
[2] Chen, A. et al., 2007, “Idiopathic membranous nephropathy in pediatric patients: presentation, response to therapy, and long-term outcome.” BMC Nephrology, 8:11
[3] Filler, G. et al., 2003, “Is there really an increase in non-minimal change nephrotic syndrome in children?”Am J Kidney Dis, Dec;42(6):1107-13.
[4] White OJ, et al.,2012. “A genomics-based approach to assessment of vaccine safety and immunogenicity in children.”Feb 27;30(10) PMID 22230586
_______________________________________________________________________________________________________________________________
About the author: Dr. Suzanne Humphries is a conventionally educated medical doctor who has taken the walk into, around, and out of the allopathic paradigm. She fully and successfully participated in the conventional system for 19 years, witnessing first-hand how that approach fails patients and creates new disease time and again. Prior to medical school, she earned a bachelor’s degree in physics from Rutgers University. After two years as the head technician in a research biochemistry lab, she went to medical school, graduating from Temple University School of Medicine in 1993. She then studied internal medicine in the Bronx, NY where she completed her 3-year medical residency. At this juncture, Dr Humphries became more aware of the failures of primary care medicine, observing that doctors are largely trained to prescribe drugs and hunt down disease. Despite this approach, the patients continued to get sicker, requiring more drugs and ultimately developing degenerative diseases. Not wanting involvement in the generation of chronically ill patients, she opted to work at the other end of the allopathic continuum and completed a fellowship in Nephrology. After 14 years of practicing allopathic kidney medicine, her perspective on the overall success of the allopathic paradigm has developed and matured. She views allopathic medicine as an overused system- that when implemented as first line treatment across-the-board for mild illnesses and symptoms, will mostly just drive chronic illnesses deeper and more seriously into the patient.
Dr. Humphries has re-dedicated her life as a doctor. She recently moved beyond mainstream medicine, and is utilizing nontoxic means to help restore health in those who seek her assistance. Homeopathy, nutrition, micronutrients, and detoxification are among the modalities she implements. Dr. Humphries is on the board of directors of the International Medical Council on Vaccination. She lives in Maine, USA.
- See more at: http://www.vaccinationcouncil.org/2012/03/09/common-vaccine-ingredient-implicated-in-nejm-article-as-causative-in-serious-type-of-kidney-disease-by-suzanne-humphries-md/#sthash.u2gPcVlh.dpuf
