
|
|

Women's Information Network Against Breast Cancer http://www.winabc.org. Fri Oct 15 13:56:11 2004 Pacific Time
Hidden Epidemic of Monkey Virus Infections Arose From Contaminated Polio Vaccines, Researcher Says
ROSEMEAD, Calif., Oct. 15 (AScribe Newswire) -- The Centers for Disease Control and Prevention (CDC) was recently notified of an individual infected with a monkey cytomegalovirus. Previous reports to CDC of infections with viruses that originated from African green monkeys have largely gone ignored, according to Dr. W. John Martin, M.D., Ph.D., founder of the privately funded Centers for Complex Infectious Diseases in Rosemead, California. "Public health officials have been very resistant, since any airing of this topic will lead to the inevitable conclusion that the government erred in accepting cytomegalovirus contamination of the African green monkeys used in polio vaccine production."
In a 1972 joint government-industry study cited by Dr. Martin, cell cultures from all 11 monkeys studied were contaminated with simian cytomegalovirus. The scientific community was not informed of this finding. In spite of industry's efforts to curtail contamination, Food and Drug Administration (FDA) officials have confirmed that 3 of 8 licensed polio vaccines released in 1976 have DNA of simian cytomegalovirus. Martin referred to these results in an October 2002 meeting of the Institute of Medicine. His manuscript entitled "DNA Analysis of a Stealth-Adapted Simian Cytomegalovirus" was removed from the published proceedings of the conference.
Martin contends that many of the diseases of epidemic proportions in this county, including autism and attention deficit hyperactivity disorder in children, as well as cancer, chronic fatigue, fibromyalgia and Alzheimer's-like illnesses in adults, are caused by stealth-adapted viruses.
Stealth-adaptation is a process whereby cell-damaging viruses lose components that are normally targeted by the immune system. Some, but not all stealth-adapted viruses are derived from simian cytomegalovirus. Increasingly, Martin is hearing of family illnesses of presumptive infectious origin. He recently submitted a manuscript entitled "Complex multi-system illnesses occurring within a family: Presumptive evidence for an infectious disease process" to the CDC Journal of Emerging Infectious Diseases, but its publication was declined. "It is hard to wake them up" says Martin "and near impossible to break through the self protective barrier of those who recognize that cytomegalovirus contaminated polio vaccines used in Central Africa could have triggered the formation of the AIDS virus. CDC has a collection of sera from polio vaccine immunized African children that, under better leadership, would have been tested for cytomegalovirus antibodies." Except for legal purposes, Martin has been prohibited from communicating results of stealth virus testing to individuals with complex unexplained illnesses. A petition recently sent to CDC requesting that it tests autistic children for stealth-adapted viruses was seemingly futile.
"The real tragedy of CDC," says Martin "is the public's expectation that it will aggressively pursue every indication of potentially infectious agents contributing to human diseases. Doing nothing is tantamount to allowing disease to go unchecked. One way to establish dialogue with the CDC is through the litigation process. Alternatively, a Congressman or Senator willing to risk the ire of the pharmaceutical industry must insist that CDC immediately address the issue of cytomegalovirus contamination of polio virus vaccines and interview some of the many patients infected with stealth-adapted viruses."
Dr. Martin says, "Now is the time for well designed clinical studies to evaluate methods to prevent disease transmission and to help restore normal brain function to stealth-adapted virus infected individuals. The public needs to be informed and our Government agencies need to respond."
More information, including copies of the manuscripts submitted to the Institute of Medicine and CDC Journal of Emerging Infectious Diseases, is available at www.s3support.com
CONTACT: W. John Martin, M.D., Ph.D., Director, Center for Complex Infectious Diseases, Rosemead CA 91770, 626-616-2868, s3support@email.com
BIO/C.V.
W. John Martin
Education
o University of Sydney Australia . Graduated B.Sc. (Med) in 1963 and M.B., B.S. (M.D. equivalent) in 1965.
o Medical Residency at Royal Prince Alfred Hospital, Sydney, Australia 1965-1966.
o University of Melbourne . Ph.D. in Immunology 1967-1979.
o Post-doctoral training at the National Institutes of Allergy and Infectious Diseases, NIH (1970); Pathology Department, Harvard Medical School (1971), National Cancer Institute, NIH (1972) and University College London (1973-1974).
o Pathology Residency, National Naval Center, Bethesda Maryland (1980-1985)
Academic Appointments
o Visiting Scientist and Expert National Cancer Institute, NIH, Bethesda , MD 1/71-9/72; 2/74-1/76
o Supervisory Medical Officer GS-14 and Head, Oncology Unit, Division of Virology, Bureau of Biologics, Food and Drug Administration, NIH, Bethesda, MD 1/76-2/81
o Supervisory Medical Officer GS-15 and Head, Biological Resources Branch, Biological Response Modifiers Program, National Cancer Institute, NIH, Bethesda , MD 3/81-1/82
o Associate Professor of Pathology, Uniformed Services, University of the Health Sciences, Bethesda , MD 1/82-6/85
o Professor of Pathology, University of Southern California School of Medicine 7/85 - present. Tenured position with leave granted from 1996.
Clinical Appointments
o Chief of Immunology/Immunopathology Unit, Section of Laboratories and Pathology, Los Angeles County + University of Southern California Medical Center, Los Angeles , CA 7/85-6/93. Unit name change to Immunology/Molecular Pathology 7/88. Director of Flow Cytometry, 6/93 to 10/95
o Director of USC Infectious Diseases Laboratory and of USC Molecular Pathology Laboratory within the USC Clinical Laboratories, USC School of Medicine 1/88-10/95
Other Positions
o Founder and Director, Center for Complex Infectious Diseases, Rosemead, California 91770 (A research and clinical laboratory testing facility supported by donations and other funding managed by the National Heritage Foundation)
Board Certification
o Diplomat of the American Board of Medical Laboratory Immunology 1983
o Diplomat of the American Board of Pathology in Anatomic and in Clinical Pathology 1984
o Special Competence Certification in Immunopathology, American Board of Pathology, 1984
o Special Competence Certification in Medical Microbiology, American Board of Pathology 1985
Media Contact: W. John Martin, M.D., Ph.D., Director, Center for Complex Infectious Diseases, Rosemead CA 91770, 626-616-2868, s3support@email.com
J Autism Dev Disord. 2004 Oct;34(5):583-6.
Brief report: autistic disorder in three children with cytomegalovirus infection.
Sweeten TL, Posey DJ, McDougle CJ.
Department of Psychiatry, Indiana University School of Medicine, Indianapolis, IN 46202-4800, USA.
Previous research has identified a relationship between autistic disorder (autism) and specific congenital infections. Three cases of congenital or perinatal cytomegalovirus (CMV) infection occurring in association with autism are described. Hypothetical mechanisms relating congenital infection, such as CMV, to the development of autism are discussed. A better understanding of the immunologic response to certain congenital infections may provide important information pertaining to the pathophysiology and etiology of autism in vulnerable individuals.
SCIENCE JOURNAL
Medscape Medical News
Risk of Neurologic Abnormalities High in Prenatal CMV Infection
http://mp.medscape.com/cgi-bin1/flo?y=aWdA0D86Go0DzT0FN250AO
Laurie Barclay, MD
Sept. 9, 2002 — The neurologic outcome of primary maternal cytomegalovirus (CMV) infection is bleak, according to a report published in the September issue of Obstetrics and Gynecology. Even in women who chose not to abort, 19% of infants had postnatal neurologic abnormalities despite negative prenatal ultrasound.
"Positive isolation of CMV accompanied by positive polymerase chain reaction (PCR) values in amniotic fluid provided approximately 94% certainty of in utero CMV infection," write Shlomo Lipitz, MD, and colleagues from Tel Aviv University in Israel. "The risk of postnatal neurologic abnormalities was 19% (3 of 16) when there were no prenatal ultrasonographic abnormalities."
Among 50 pregnancies (51 fetuses) with proven primary maternal infection and vertical transmission of CMV, 33 women (66%) elected pregnancy termination. Ultrasound documented fetal abnormalities in 11 (21.5%) fetuses. Two of these continued to term. Both were congenitally infected, and one had neurologic abnormalities. Of 17 pregnancies (18 fetuses) which continued to term, four fetuses had neurologic abnormalities, and three of these had normal prenatal ultrasound. The remaining 14 had normal prenatal ultrasound and no postnatal neurologic abnormalities.
"The severity of the sonographic abnormalities probably plays an important role in prognosis," the authors write, recommending additional and larger studies. "The significance of mild signs of fetal infection, e.g. hyperechogenic bowel, in the presence of maternal infection is still unknown."
Obstet Gynecol. 2002;100:428-433
Reviewed by Gary D. Vogin, MD
Live Oral Poliovirus Vaccines and Simian Cytomegalovirus
Biologicals Volume 30, Issue 3, September 2002, Pages 167-174
Ana M. Sierra-Honigmann and Philip R. Krausef1
Center for Biologics Evaluation and Research, Food and Drug Administration, Building 29A Rm 1C16 29 Lincoln Drive, Bethesda, MD 20892, U.S.A.
Received 6 July 2001; accepted 5 February 2002. Available online 5 September 2002.
Abstract
Live oral poliovirus vaccines (OPV) are often produced in primary Cercopithecus monkey kidney (CMK) cells. The kidneys of these monkeys are often latently infected with simian cytomegalovirus (SCMV), and CMK cultures are frequently contaminated with SCMV. We tested human, monkey and rabbit tissue culture systems, and found that MRC-5 cells are most sensitive for detection of SCMV. To address the question of whether OPV could be contaminated with infectious SCMV, we inoculated MRC-5 cells with neutralized OPV manufactured in the United States between 1972 and 1998. Infectious SCMV was not found in any of the vaccine lots tested. We also used the polymerase chain reaction (PCR) to search for SCMV DNA in live oral poliovirus vaccines; SCMV DNA sequences were found in several of the vaccine lots manufactured prior to 1992.
Simian cytomegalovirus and contamination of oral poliovirus vaccines
Biologicals Volume 31, Issue 1, March 2003, Pages 63-73
Sally A. Baylis, , a, Nita Shaha, Adrian Jenkinsb, Neil J. Berryb and Philip D. Minora
a Division of Virology, National Institute for Biological Standards and Control, Blanche Lane, South Mimms, Potters Bar,Hertfordshire EN6 3QG, UK
b Division of Retrovirology, National Institute for Biological Standards and Control, Blanche Lane, South Mimms, Potters Bar,Hertfordshire EN6 3QG, UK
Received 27 August 2002; accepted 15 October 2002. ; Available online 28 February 2003.
Abstract
In the 1950s the use of primary rhesus macaque kidney cultures to propagate poliovirus for vaccine production led to the contamination of vaccines with simian virus 40 (SV40). African green monkey kidney (AGMK) cultures free of SV40 were used as an alternative cell substrate for vaccine manufacture. In this study we evaluate oral poliovirus seeds, vaccine bulks and vaccines themselves for the presence of a common contaminant of AGMK cultures, simian cytomegalovirus (SCMV). Using sensitive polymerase chain reaction (PCR) techniques, nearly half of the samples analysed were found to be contaminated with SCMV sequences. However, vaccine bulks, positive by PCR for SCMV failed to show any evidence of infectious virus in these studies. One poliovirus vaccine and one seed, propagated on rhesus macaque kidney cultures were found to be positive for the rhesus monkey CMV by PCR.
By KATRINA WOZNICKI, UPI Science News
BIRMINGHAM, Ala. (UPI) - A common human virus might have some role in the development of colon cancer, according to a new, small study released Thursday.
Preliminary findings from researched conducted at the University of Alabama in Birmingham suggest the cytomegalovirus, or CMV, a widespread organism particularly dangerous to people with weakened immune systems, could be associated with the cellular breakdown that leads to colon cancer. "This virus is strongly associated with malignant brain tumors," lead researcher Dr. Charles S. Cobbs, also a neurosurgeon with the Birmingham VA Medical Center, told United Press International. "The more I learned about virus, the more I realized it had many properties important for cancer in general."
As described in the Nov. 16 issue of the British journal The Lancet, Cobbs and his team took colorectal polyps, tumors and surrounding healthy cells from 29 patients. They found proteins from the cytomegalovirus in approximately 80 percent of the polyps and in about 85 percent of the colon cancer samples.
"I'm not trying to say this virus is causal in colon cancer," Cobbs said." I've just made a preliminary observation ... whether or not it's influencing the cancer remains to be determined." The virus might be inducing unwanted cell behavior that could lead later to uncontrollable cell growth or cancer, Cobbs explained, but more study is needed to confirm these findings.
Cytomegalovirus resides in about 50 to 80 percent of the U.S. population, Cobbs said, and age and socioeconomic status are risk factors. The virus also can cause ulcers, he explained. It is a relative of the herpes virus and, like herpes or chicken pox, when an individual contracts it the virus cannot be eradicated. It can lie dormant in a person for years or even decades and not cause any harm.
In people with compromised immune systems, however, such as AIDS or chemotherapy patients, the virus can wreak havoc on the gastrointestinal tract, the eyes and the brain, Cobbs said.
Although the virus is common, Cobbs said people should not be worried about getting cancer from it. "There's probably at least 15 coincidental things that all have to occur at once" involving this virus before cancer develops, he said.
Viruses have been implicated in cancers before, but Dr. Gerard Blobe, an assistant professor of medicine in pharmacology and cancer biology at Duke University Medical Center in Durham, N.C., said previous studies on the cytomegalovirus have been mixed or inconclusive.
"It would be a little surprising" if these findings proved to be true, he told UPI. "They've certainly been looking for causes of colon cancer. It is surprising just because it goes in contrast in what other investigators have shown, but have not really reported."
In fact, Blobe said of the herpes virus family, cytomegalovirus is thought to be one that does not influence cancer. "I think this study would need to be investigated in larger population of individuals before we truly believe this is a cause for colon cancer," he said.
FRIGHTENING BUT FANTASTIC NEWS!
First, The Bad News
It is very bad. People who live in North America are at a far greater risk today of contracting anything from colds to cancer, from headaches to heart attacks, than they were last year! The immune system is the main link to most health problems. The stronger the immune system, the less risk people have of any disease. The weaker the immune system, the greater the risk of getting any disease. Everyone develops cancer cells on a daily basis, and viruses and bacteria are probing our defenses every minute.
How bad is it? Your Natural Killer Cells (NKC) are the most active part of your immune system, and are your first line of defense against bacteria, viruses, and cancer. Between 1981 and 1991, Natural Killer Cells in the average American declined 1% a year—from 1991 to 1997, the loss accelerated to 3% a year, a 26% drop in just 16 years! A bad night's sleep can lower it another 30% for a day or two. Several spoons of sugar from soft drinks and goodies can lower it another 50% for up to five hours—all day for the many who indulge their "sweet tooth" several times a day. Tests of dieters saw a drop of 50%! (Dieters who exercised 40-60% maximal intensity did not suffer this loss—but all who exercise strenuously for more than an hour have more infections in the next week.) Ill people run a very low NKC count, inviting further illness. Many drugs and opiates interfere with the immune system [opiates increase apoptosis (cell death) of T–lymphocytes from the norm of 5% to 30%]. As a result, death by infections other than HIV has increased 22%!
"Researchers have shown for the first time that people who developed the fatty blockages that mark heart disease had an infection first...Many studies have linked heart disease with infections by bacteria or viruses...several teams have found Chlamydia Pneumoniae in the hardened plaques blocking the arteries, as well as Helicobacter pylori...and a virus known as cytomegalovirus (herpes-5)." Chlamydia pneumoniae, which infects sinuses, was found in 17 of 19 Alzheimer's victims' brains! Viruses cause blood to sludge, causing clotting which can lead to strokes within the following two weeks. Encephalitis is caused by the West Nile and St. Louis viruses, enteroviruses, herpes, varicella, LaCrosse, and James Canyon viruses. Some are mosquito-transmitted; others, such as herpes, are spread person-to-person. Lipkin, in 1995, found small RNA horse microbes, called borna viruses, in the brains of people who had suffered from either schizophrenia or bipolar disorder. It has been implicated in some forms of depression, and several laboratories have shown that the hardy microbes thrive for decades in the bodies of unfortunate human beings. Additionally, a second virus, toxoplasma gondii, has been found in people with Schizophrenia. This is the cat virus acquired from handling cat feces. Human pavrovirus B19 has been linked to arthritis, MS, and Sickle Cell Anemia. Breast cancer tissue in far higher percentage (33%) than healthy breast tissue (2%) contains a retroviruses identical with mouse mammary tumor virus!
Dr. Hans A. Nieper, renown German researcher, and associates, completed a four year tracking program that convinces them there is aggressive, viral activity in 90% of all malignancies, colitis, rheumatoid arthritis, scleroderma, multiple sclerosis, and Lou Gehrig's disease (ALS). He concludes that a virus is active in most diseases. He tracked Herpes I and II and the cytomegalovirus (Herpes–V). He considers the cytomegalovirus to be particularly problematic as it replicates in the lymph cells and leaves its genetic information there to disrupt normal cellular information for years to come. HSV-I occasionally travels to the brain and kills (R. L. Ashley, UW School of Medicine). Researchers at the University of California recently identified a virus in ALS. The bacteria, mycoplasma, infests the joints in rheumatoid arthritis, and salmonella and Lyme disease can trigger an autoimmune attack on joints. Measles virus is found in the colon of Autism and Crohn's. Parasites were found in 93% of Chronic Fatigue Immune Deficiency Syndrome (CFIDS) (J Nutritional Med, 1990; 1:27-31) and in many with seizures.
The Coxsackie virus is implicated in many diseases (Type I, juvenile diabetes). In the USA, the retrovirus sickens 3,000,000 children, sending 500,000 to the doctor and 75,000 to the hospital because formula does not provide the needed substrate (found in Mother's milk) for the glycoprotein, Lactadherin, that coats the virus preventing it from infecting cells (David Newburg Ph.D., Shiver Center for Mental Retardation, Massachusetts). A type of retrovirus is involved in HIV, Lupus, and other diseases. Helicobacter pylori has been implicated in 95% of ulcers, in gastritis, excessive stomach acid, stomach cancer, heart disease, and possibly certain allergies. Herpes Virus–VI has been identified in the brain (73%) and blood (56%) of Multiple Sclerosis patients. Viruses act to "trigger" other diseases in prone individuals. Many bacteria have become resistant to our most powerful antibiotics.
This means that not just some of us, but all of us are at great risk to diseases. Close to 100% of us have heart disease that began when we were children—it just takes 40 years to develop. Of the teenagers who died during the Viet Nam war, 100% had signs of clogging arteries! No one is fully healthy any more, not even if you look and feel healthy and your doctor says your blood test is great! Dr. Harry Alsleben has shown that blood tests will not predict imminent death, nor will they change after death! How can they predict health?
Here's further evidence: 50% of all deaths in America are from circulatory/heart disease, 33% from cancer, and 12% from diabetes (that's 95%). These were rare conditions just decades ago. In addition, we now have rampant allergies, arthritis, asthma, Autism, Chronic Fatigue, Fibromyalgia, antibiotic resistant bacteria (some of which actually eat antibiotics), and many very dangerous mutant viruses.
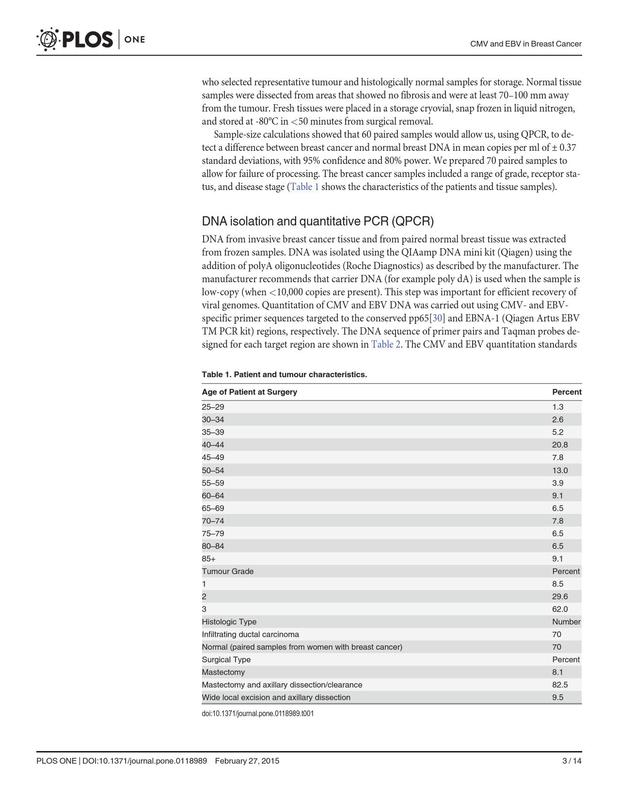
J Pathol 2002 Jul;197(3):395-402
Related Articles,Links Herpesviruses in brain and Alzheimer's disease.
Lin WR, Wozniak MA, Cooper RJ, Wilcock GK, Itzhaki RF.
Department of Optometry and Neuroscience, UMIST, Manchester, UK.
It has been established, using polymerase chain reaction (PCR), that herpes simplex virus type 1 (HSV1) is present in a high proportion of brains of elderly normal subjects and Alzheimer's disease (AD) patients. It was subsequently discovered that the virus confers a strong risk of AD when in brain of carriers of the type 4 allele of the apolipoprotein E gene (apoE-epsilon4). This study has now sought, using PCR, the presence of three other herpesviruses in brain:human herpesvirus 6 (HHV6)-types A and B, herpes simplex virus type 2 (HSV2)and cytomegalovirus (CMV). HHV6 is present in a much higher proportion ofthe AD than of age-matched normal brains (70% vs. 40%, p=0.003) and there is extensive overlap with the presence of HSV1 in AD brains, but HHV6, unlike HSV1, is not directly associated in AD with apoE-epsilon4. In 59% of theAD patients' brains harbouring HHV6, type B is present while 38% harbour both type A and type B, and 3% type A. HSV2 is present at relatively low frequency in brains of both AD patients and normals (13% and 20%), and CMVat rather higher frequencies in the two groups (36% and 35%); in neither case is the difference between the groups statistically significant. It is suggested that the striking difference in the proportion of elderly brains harbouring HSV1 and HSV2 might reflect the lower proportion of people infected with the latter, or the difference in susceptibility of the frontotemporal regions to the two viruses. In the case of HHV6, it is not possible to exclude its presence as an opportunist, but alternatively, it might enhance the damage caused by HSV1 and apoE-epsilon4 in AD; in some viral diseases it is associated with characteristic brain lesions and it also augments the damage caused by certain viruses in cell culture and in animals.
Copyright 2002 John Wiley& Sons, Ltd.
PMID: 12115887 [PubMed - indexed for MEDLINE]
http://www.immunesupport.com/library/showarticle.cfm/ID/3547/
Stealth Virus Infected Children: Brain Damage and the Development of Chronic
Fatigue Syndrome and Fibromyalgia
ImmuneSupport.com
05-06-2002
W. John Martin, M.B., B.S., Ph.D. Center for Complex Infectious Diseases 3328 Stevens Avenue, Rosemead, California USA 91770 e-mail ccidlab@hotmail.com Abstract Atypically structured, vacuolating cytopathic stealth viruses exist and can induce multi-system illnesses, including severe brain disease. DNA sequencing studies on an African green monkey simian cytomegalovirus (SCMV)-derived stealth virus has heightened concerns for the potential devastating effects of stealth viruses on living organisms. The prototype stealth virus has lost the major antigenic targets for recognition by cytotoxic T lymphocytes. More impressively, it has captured, amplified and mutated both cellular and bacterial genetic sequences. The term "viteria" has been introduced for viruses containing bacterial sequences. Stealth viruses have been cultured from babies born to infected mothers and from children with a variety of neurological, psychiatric, allergic and neoplastic diseases. The cytopathic changes seen in stealth virus cultures correlate well with the vacuolating cellular damage observed on histological sections of brain tissues obtained on biopsy and on autopsy. Studies to combat the spread of stealth viruses and to effectively treat those already infected are clearly warranted. Additional information is available from the internet at
- www.ccid.org Poliovirus Vaccine Contamination One of society's highest obligations is the protection of its children. Vaccine programs provide a proven method for childhood disease prevention. The safety of such programs has been entrusted to vaccine manufacturers and to government regulatory agencies. Although widely touted as the major medical triumph of the 20th century, the development of viral vaccines has elements of less than stellar performance. The discovery in 1960 of live SV-40 virus contamination in formalin-treated poliovirus vaccine, produced in kidney cells cultures from rhesus monkeys, did not lead to an immediate recall of the contaminated vaccines. Rather, the production method was switched to the use of kidney cells from the less well characterized African green monkeys. This switch in monkey species was soon followed by the decision to forgo formalin inactivation by using a weakened (attenuated) live strain of poliovirus (1). Persisting concerns regarding contaminating viruses in the live poliovaccine led in 1972 to a joint study between the vaccine manufacturer and the United States Food and Drug Administration (FDA). Kidney cultures from all 12 monkeys tested grew African green monkey simian cytomegalovirus (SCMV). Only 4 of the SCMV isolates were detectable using the regular methods for virus detection (2). No changes in testing methodology were imposed, nor was the scientific community alerted to the findings. An explanation that was subsequently offered was that information about the study was deemed to be proprietary. The results of this earlier study were, however, not even conveyed to FDA scientists who, in 1977, notified the Director of the FDA's Bureau of Biologics that certain poliovaccine lots contained unexplained non-cellular DNA; and were, therefore, potentially virally contaminated. The issue of SCMV contamination of poliovirus vaccines was again raised with the FDA in May 1995. I was then working as a virologist at the University of Southern California. I had developed tissue culture methods that clearly indicated the presence of atypical viruses in patients with complex neurological diseases (3-7). The viruses were striking in that they failed to evoke an inflammatory reaction in the patients from whom they were isolated. They were termed stealth viruses on this basis, and seemingly they lacked target antigens for recognition by the body's cellular immune system. Sequencing studies on a stealth virus strongly suggested it had originated from SCMV. Several meetings with FDA and Center for Disease Control and Prevention (CDC) officials pointed to their unwillingness to allow any outside review of vaccine safety procedures. For example, a simple request to review histological slides of neurological tissue of monkeys inoculated with poliovaccine was refused, again on the basis that it was proprietary information. Noteworthy was the admission that the vaccines were routinely tested in rhesus monkeys because African green monkeys commonly show evidence of neurological disease. Moreover, even in rhesus monkeys, the vaccine was said to induce considerable neurological damage, although less than that induced by non-attenuated poliovirus. The actual SCMV-related sequence data were published in a respected virology journal in July 1995 (8). The article aroused the interest of anti-vaccine consumer groups. Through the efforts of one of these groups, I was invited to attend a vaccine safety meeting of the Institute of Medicine, National Academy of Sciences (9). The open meeting held on November 6, 1995 was followed the next day by an "executive session." I was later informed that several Industry-connected individuals at this meeting were "furious" that I was allowed to speak. A "watered down" account of what I said subsequently appeared in the official report of the meeting. Some insight into the lack luster nature of the existing regulatory system was provided by several brief interchanges with Government and other officials during the last several years. For example, I was asked whether formalin treatment would inactivate stealth viruses. My response was that I did not know. The chairman of the National Immunization Advisory Committee suggested the advocacy of a split protocol in which both formalin inactivated and live attenuated poliovaccine would provide the necessary time window for the manufacturer of the inactivated vaccine to develop the stocks required for a complete switch. True to his suggestion, the official switch to inactivated vaccine is scheduled for January 2000. Of course, those "in the know" would have already switched to the inactivated vaccine. An FDA reform bill was being considered by Congress in 1997. I suggested that the bill include the provision that "If a safety issue is identified in the regulation of a biological product, then Industry would waive its proprietary protection so that the information could be made available to the scientific community." The suggestion was well received by the counsel for the House Commerce Committee. It was soon dropped, however, when support was not forthcoming from Industry, FDA or the American Medical Association (AMA). In speaking with an AMA lobbyist, I understood they "would not want the public to know that their doctors were not in the knowledge loop." I once asked industry personnel involved in poliovaccine production whether they were still encountering SCMV in poliovaccine production lots. After some hesitation that disappeared as we all identified ourselves as parents, the straightforward answer was "not infrequently." Armed with this information I again requested an FDA official to please use modern techniques, such as the polymerase chain reaction (PCR), to screen poliovaccine lots for SCMV. "We would not know what to do with a positive result" was his answer. Sequencing Studies on the SCMV-Derived Stealth Virus Continued sequencing of the prototype SCMV-derived stealth virus have helped substantiate the original suggestion that stealth adapted viruses lack the critical target antigens for cellular immune recognition (10-11). The virus has a fragmented viral genome (11). While the various fragments cover extensive regions of a typical cytomegalovirus, it is missing sequences that correspond to the known major viral antigens targeted by anti-cytomegalovirus cytotoxic T lymphocytes. Other regions of the cytomegaloviral genome are unevenly distributed, with certain viral genes being markedly over represented. When multiple copies of a gene were identified, it was not uncommon to see minor sequence differences indicating an "error-prone" replication process (10-11). An overview of the viral sequence data is that approximately two-thirds of the clones contain sequences that correspond to cytomegaloviral genes (10). Where direct comparisons could be made, the genetic sequences matched more closely to rhesus monkey cytomegalovirus than to human cytomegalovirus. Even closer homology could be shown between the stealth virus and the limited known sequences of SCMV. The data are unequivocal that the virus had originated from an SCMV and hence from a poliovaccine (8,10-11). The question that arose was how could such a fragmented viral genome, lacking certain viral genes while over expressing other viral genes, retain and/or regain its ability to be cytopathic for cells. A partial answer to this question came from analyses of the genes that did not correspond to those of a cytomegalovirus. Several genes were apparently directly incorporated from infected cells. These genes frequently contained short stretches of highly reiterated cellular sequences (12). One set of cellular genes was particularly noteworthy. They corresponded to three copies of a gene that encode a chemokine (13). While the cellular DNA for this gene contain introns, the assimilated genes were lacking introns and had, therefore, been 'captured" as RNA sequences. This finding provided direct evidence for reverse transcription (that is RNA to DNA) in the reconstruction of cytopathic stealth viruses. This process was consistent with the error-prone replication of the stealth virus. Among the cellular genes identified within the stealth virus, were also genes with potential oncogenic (cancer causing) activity (13). This finding highlighted ongoing observations that stealth adapted viruses were being repeatedly detected in both children and adults with various cancers (14 and unpublished observations). An additional challenging observation was the finding that some of the incorporated sequences had clearly been captured from bacteria (15). The bacterial genes covered a wide range of metabolic functions that could enhance bacterial growth (16). This observation was soon followed by the detection of atypical bacteria within the flora of stealth virus infected patients. Moreover, infectious agents could be released from such bacteria and cause cytopathic effects when transferred to human and to animal cells. The presence of bacterial sequences within viruses infectious for human and animal cells represents a novel life form that has been termed viteria. The prospect exists for metabolically empowered bacteria to establish an increasing presence within nature with potentially devastating biological consequences. The notion that viteria represents "Nature's biological weapons program" is not too far fetched. Information concerning the existence of viteria and their potential Public health consequences was conveyed to CDC, FDA, NIH and the US Congress. Responses are still being awaited from these agencies. Viteria: An Explanation for Serological and Molecular Findings of Multiple Pathogens in Adults and Children with Chronic Fatigue and Related Illnesses The recombination of viral, bacterial and cellular genes within broadly infectious viteria could help explain much of the confusion surrounding the cause of chronic fatigue like illnesses in adults, children and household pets. Depending upon the focus of the research, various investigators have ascribed these illnesses to different types of pathogens. Some of the early reports relied upon high antibody titers to Epstein-Barr virus (a type of herpesvirus). Others have noted antibodies reactive with human herpesvirus-6, human herpesvirus-7, human T lymphotropic virus, parvovirus, Borna virus, modified endogenous retroviruses, enteroviruses, including poliovirus, and hepatitis C viruses (17-25). Using molecular techniques, data have been obtained suggesting the presence of mycoplasma species, Chlamydia, Rickettsiae, Brucella and even Borrelia bacteria (26-30). These data are consistent a broad family of viteria that have, and are continuing to, capture, amplify and mutate viral, cellular, bacterial and even fungal genes. Among the cellular/viral genes are likely to be genes encoding the reverse transcriptase of endogenous retroviruses. Although, infection can pass between individuals, including human: animal transmissions, via infected bacteria, the primary brain associated illness is viral not bacterial. The apparent clinical benefits that may occur following antibiotic therapy are potentially explainable by the known capacity of certain antibiotics to modulate chemokine mediated viral activation and replication. Viteria Detection Systems The molecular diversity of viteria has helped underscore the value of tissue culture as a primary detection assay. In a relatively straightforward procedure, cells from patients are incubated with normal human and/or animal fibroblasts. The cultures are observed for the development of a vacuolating cytopathgic effect (CPE). For controls, blood samples are obtained from healthy blood donors. None of the controls are expected to yield a positive CPE. In contrast, stealth virus infected patients will typically yield a clearly positive culture. Once established, the cultures can be screened using various immunological and molecular based assays. In particular, cells undergoing CPE will typically stain with polyclonal antisera reactive with various herpesviruses. Similarly, low stringency polymerase chain reaction (PCR) will typically yield multiple products that can be isolated, cloned and sequenced. Semi-quantitative cultures can also be used to assess efficacy of various therapies including chemokine modulating agents and anti-viral drugs. It is also appropriate to screen the bacterial flora of infected individuals for atypical bacteria. If necessary, these can be treated directly using antibiotics and probiotics. Clinical Studies During the last decade, I have written several clinical articles describing stealth virus infected patients with complex illnesses. The patients have included children with autism, adults with psychotic disease and several individuals with chronic fatigue/fibromyalgia syndrome. Many of the articles had been summarily dismissed when submitted to major medical journals. The suggestion of a linkage to vaccine use or of community wide epidemics has been unsettling to many reviewers. Still the work has appeared in peer reviewed publications and has been presented at various meetings (31-36). For example, a recent publication (36) described a stealth virus infected child whose illness began in 1997 as a behavioral problem. It took over seven months before the illness was attributed by his parents, both of whom were physicians, to brain damage. Even then a qualified neurologist was unable to detect impaired motor or sensory functions. Yet magnetic resonance imaging (MRI) confirmed extensive sub-cortical brain damage. A brain biopsy showed marked vacuolating/spongiform change. The child's clinical condition progressively deteriorated. He was examined at several major medical centers where it was wrongly concluded that he had a genetic disease from which he would soon die. He was shown to be stealth virus infected by tissue culture and significantly improved with ganciclovir therapy, although he still had major residual deficits. In spite of several courses of anti-viral therapy, with and without steroids, he subsequently succumbed to overt cerebral swelling and herniation. Other fatal cases have included a young adult initially diagnosed as having a psychotic illness. Four years into this illness, she had an acute exacerbation with coma and massive brain damage (32). Her cerebrospinal fluid grew out a stealth virus closely related to that of the prototype SCMV-derived virus. Another patient with a fatal illness and positive CSF findings died with evidence of a cerebral vasculitis (33). Virally infected newborn children have variously presented with an acute viral-like syndrome with hepatomegaly, thrombocytopenia, choroid plexus hemorrhage or with more subtle changes comprising unexplained seizure activity and/or delayed neurological development. At least one child, born to a mother with a chronic fatigue like illness, died from a sudden infant death syndrome, two weeks following routine vaccination. Young children have presented with autism, attention deficit and hyperactivity, learning and other behavioral disorders. The association of stealth virus with autism was clearly established in controlled double blind studies. Whereas none of 19 control blood samples tested positive, 13 of 18 children with autism yielded repeated positive stealth virus cultures. Other culture positive clinical groups have included in-patients in psychiatric institutions, cancer patients, including essentially 100% of patients diagnosed with multiple myeloma, auto-immune illnesses, including systemic lupus erythematosus, rheumatoid arthritis and multiple children diagnosed as having chronic fatigue syndrome. With all of these illnesses, stealth viral infection is viewed as a major contributing factor, complicated by the overlay of auto-immune, allergic and/or neoplastic processes. Conclusions An essential theme of this presentation is the apparent lack of responsiveness on the part of those entrusted with the nation's Public Health. While it can be argued that adults need to compete for allocated resources applied to various illnesses, it is difficult to understand the indifference shown to health issues affecting children. Where is the concern that a biopsy-proven childhood viral infection was not recognized at major medical centers? Where is the interest in the many other children who have tested positive for stealth viruses? Why the lack of discussion about possible brain damage causing national tragedies such as school shootings, and the increasing prevalence of autism, attention deficit, asthma and sudden infant death syndrome? Are stealth virus infected patients populating our psychiatric institutions, allergy clinics and even our cancer wards? The world and, in particular, its children appear to be at risk for stealth adapted viruses. The contribution of vaccines to the formation and dissemination of these viruses should be an open topic for scientific discussion. This is not occurring with those presently in charge of overseeing the safety of the Nation's immunization program. References 1. Paul JR. A history of poliomyelitis. Yale University Press, New Haven, 1971. 2. Unpublished documentation. 3. Martin W.J. Viral infection in CFS patients. in "The Clinical and Scientific Basis of Myalgic Encephalomyelitis Chronic Fatigue Syndrome." Byron M. Hyde Editor. Nightingale Research Foundation Press. Ottawa Canada pp 325-327, 1992. 4. Martin WJ, Zeng LC, Ahmed K, Roy M. Cytomegalovirus-related sequence in an atypical cytopathic virus repeatedly isolated from a patient with chronic fatigue syndrome. Am J Pathol. 1994;145:440-51. 5. Martin WJ. Stealth viruses as neuropathogens. CAP Today. 1994 ;8:67-70. 6. Martin WJ, Glass RT. Acute encephalopathy induced in cats with a stealth virus isolated from a patient with chronic fatigue syndrome. Pathobiology. 1995;63:115-8. 7. Martin WJ. Stealth virus isolated from an autistic child. J Autism Dev Disord. 1995;25:223-4. 8. Martin WJ. Presentation to the Institute of Medicine Meeting on Vaccine Safety, November 6th, 1995. Web site www.ccid.org 9. Martin WJ, Ahmed KN, Zeng LC, Olsen J-C, Seward JC, Seehrai IS. African Green Monkey Origin of the Cytopathic 'Stealth Virus' Isolated from a Patient with Chronic Fatigue Syndrome, Clin Diag Virol 1995; 4: 93-103. 10. Martin WJ. Stealth adaptation of an African green monkey simian cytomegalovirus. Exp Mol Pathol. 1999;66:3-7. 11. Martin WJ. Genetic instability and fragmentation of a stealth viral genome. Pathobiology. 1996;6:9-17. 12. Martin WJ. Cellular sequences in stealth viruses. Pathobiology. 1998;66:53-8. 13. Martin WJ. Melanoma growth stimulatory activity (MGSA/GRO-alpha) chemokine genes incorporated into an African green monkey simian cytomegalovirus-derived stealth virus. Exp Mol Pathol. 1999; 66:15-8. 14. Gollard RP, Mayr A, Rice DA, Martin WJ. Herpesvirus-related sequences in salivary gland tumors. J Exp Clin Can Res.1996;15: 1-4. 15. Martin WJ. Bacteria-related sequences in a simian cytomegalovirus-derived stealth virus culture. Exp Mol Pathol. 1999; 66:8-14. 16. Martin WJ. Viteria: Bacterial sequences in animal and human viruses. J Degenerative Diseases 1999;1:7-10. 17. Jones JF Epstein-Barr virus and the chronic fatigue syndrome: a short review. Microbiol Sci 1988;5:366-9. 18. Di Luca D, Zorzenon M, Mirandola P, Colle R, Botta GA, Cassai E. Human herpesvirus 6 and human herpesvirus 7 in chronic fatigue syndrome. J Clin Microbiol 1995;33:1660-61. 19. Jacobson SK, Daly JS, Thorne GM, McIntosh K. Chronic parvovirus B19 infection resulting in chronic fatigue syndrome: case history and review. Clin Infect Dis 1997 ;24:1048-51. 20. Behan PO, Behan WM, Gow JW, Cavanagh H, Gillespie S. Enteroviruses and postviral fatigue syndrome. Ciba Found Symp 1993;173:146-54. 21. Bruno RL, Creange SJ, Frick NM. Parallels between post-polio fatigue and chronic fatigue syndrome: a common pathophysiology? Am J Med 1998 ;105:66S-73S. 22. DeFreitas E, Hilliard B, Cheney PR, Bell DS, Kiggundu E, Sankey D, Wroblewska Z, Palladino M, Woodward JP, Koprowski H. Retroviral sequences related to human T-lymphotropic virus type II in patients with chronic fatigue immune dysfunction syndrome. Proc Natl Acad Sci U S A 1991;88:2922-6. 23. Holmes MJ, Diack DS, Easingwood. RA, Cross JP, Carlisle B. Electron microscopic immunocytological profiles in chronic
Cytomegalovirus is present in a very high proportion of brains from vascular dementia patients.
Lin WR, Wozniak MA, Wilcock GK, Itzhaki RF. Molecular Neurobiology Laboratory, UMIST, Manchester, M60 1QD, United Kingd= om.
Neurobiol Dis 2002 Feb;9(1):82-7
We previously found that herpes simplex type 1 virus (HSV1), when present in brain of carriers of the apolipoprotein E type 4 allele is a strong risk factor for Alzheimer's disease. To find if HSV1 or certain other herpesviruses are involved in vascular dementia (VaD), we searched post mortem brain specimens from patients suffering from VaD for the presence of HSV1, cytomegalovirus (CMV), and human herpesvirus type 6 DNA, using polymerase chain reaction. We have found that a very high proportion of the VaD patients, 93% (14/15), but not of age-matched normals, 34% (10/29), harbor CMV DNA (P = 0.0002); the proportions of the patients harboring the other viruses in brain do not differ significantly from those of the normals. Further studies are needed to reveal whether or not the association of CMV with VaD is causal.
PMID: 11848687 [PubMed - indexed for MEDLINE]
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=
PubMed&list_u=ids=11848687&dopt=Abstract
Case 25-2003 — A Newborn Boy with Petechiae and Thrombocytopenia
John F. Modlin, M.D., P. Ellen Grant, M.D., Robert S. Makar, M.D., Ph.D., Drucilla J. Roberts, M.D., and Kalpathy S. Krishnamoorthy, M.D., M.B., B.S.
Related Articles in Medline
Articles in Medline by Author: Modlin, J. F.
Krishnamoorthy, K. S.
Medline Citation
Infectious Diseases
Hematology
Neonatal Medicine
Pregnancy
Presentation of Case
A newborn boy was admitted to a special-care nursery because of petechiae and thrombocytopenia.
The boy had been delivered at this hospital at 39 weeks' gestation to a 32-year-old woman who had had premature rupture of the membranes 16 hours before delivery. A single dose of penicillin was administered to the mother before vacuum-assisted delivery. The Apgar score was 9 at one minute and at five minutes. A diffuse petechial rash, most prominent on the face and trunk, was noted at delivery, and the baby was transferred to a newborn nursery.
The mother had never smoked, and she had not consumed alcohol after learning of the pregnancy. Prenatal serologic tests were negative for hepatitis B surface antigen and syphilis, positive for antibodies to rubella and for IgG antibody to cytomegalovirus (CMV; 63 arbitrary units), and equivocal for IgM antibody to CMV (1 arbitrary unit; <0.9 unit is a negative result, and >1.1 units a positive result). Ultrasonographic examination of the fetus at approximately 20 weeks' gestation revealed a focus of echogenicity within the heart and a hyperechoic bowel. Amniocentesis revealed that the chromosomes and the level of alpha-fetoprotein were normal; the fetal cells were negative for mutations in the cystic fibrosis gene. The estimated risk of Down's syndrome was 1 in 85. The mother did not have a history of febrile illness, genital lesions, or rash during the pregnancy. The family history was unremarkable on both the maternal and the paternal sides.
The infant's temperature was 36.6°C, the pulse 110 beats per minute, and the respiratory rate 48 breaths per minute. The blood pressure was 60/40 mm Hg. The weight was 2.29 kg (below the 10th percentile), the length 46 cm (between the 10th and 25th percentiles), and the head circumference 33 cm (at the 25th percentile).
On physical examination, the infant appeared well and comfortable; his features were not dysmorphic, and he was not in respiratory distress. Multiple petechial lesions were present on his face, trunk, and arms and legs and were especially numerous at the site on the head where the vacuum cup had been placed (Figure 1). No lymphadenopathy was found. The anterior fontanelle was open and flat. The eyes showed no microphthalmia, icterus, or cataracts; the retinas were not examined. The clavicles were intact, and the lungs were clear. The heart sounds were normal. The abdomen was soft; the spleen was palpable 2.5 to 3.0 cm below the left costal margin, and the liver edge 3.0 cm below the right costal margin. The arms and legs were well perfused. Muscle tone was good throughout, with appropriate Moro's and sucking reflexes.
Figure 1. Photograph of the Patient, Showing Petechiae on the Forehead.
For several hours in the nursery, the infant's heart rate was in the range of 100 to 110 beats per minute, with occasional drops to 85 beats per minute. The arterial oxygen saturation occasionally declined from 95 percent or more to about 85 percent. The results of laboratory tests are given in Table 1. The levels of urea nitrogen, creatinine, total protein, triglyceride, aspartate aminotransferase, and alanine aminotransferase were normal. Examination of a peripheral-blood smear disclosed hypochromia (++), with macrocytosis, polychromasia (+), and teardrop cells. Specimens of blood, cerebrospinal fluid, and urine were obtained for culture, and ampicillin, tobramycin, and acyclovir were given. Breast-feeding was begun. The next day, the oxygen saturation ranged from 93 to 98 percent while the patient was breathing ambient air.
A diagnostic procedure was performed.
Differential Diagnosis
Dr. John F. Modlin: May we see the prenatal radiologic studies and the clinical photographs?
Dr. Susan A. Connolly (Radiology): An intracardiac focus of echogenicity, which represents a small amount of calcification, usually in the papillary muscle, was visible on a cross-section image of the fetal chest showing the oblique four-chamber view of the heart. This finding can be a normal variant; it is seen in 5 percent of normal fetuses on second-trimester scans. However, it has been associated with an approximately doubled risk of Down's syndrome. The hyperechoic bowel, which was best seen on an oblique transverse image of the abdomen, is a finding associated with infection with toxoplasma, CMV, togavirus (the agent that causes rubella), and herpes simplex virus and with increased risks of Down's syndrome, cystic fibrosis, bleeding, and growth retardation.
Dr. Stephen Walsh (Infectious Disease Unit): We were asked to see the infant the day he was born. There was a diffuse, macular, petechial eruption on his face but no pustules or vesicles (Figure 1).
Dr. Modlin: This newborn infant had intrauterine growth retardation and shortly after birth was found to have hepatosplenomegaly, thrombocytopenia, and hyperbilirubinemia. It is helpful to begin by considering the broad categories of conditions associated with thrombocytopenia in newborns (Table 2).
Table 2. Conditions Associated with Neonatal Thrombocytopenia.
Maternal antiplatelet antibodies are an important cause of thrombocytopenia in newborns, but their presence is not accompanied by hepatosplenomegaly or intrauterine growth retardation. There are no features of this case that suggest the presence of structural birth defects such as absent radii or a large hemangioma (the Kasabach–Merritt syndrome), and the complete blood count is not consistent with the presence of congenital leukemia. There are several metabolic diseases and other genetic disorders, such as Fanconi's anemia and the Wiskott–Aldrich syndrome, that may be manifested as neonatal thrombocytopenia, but usually not on the first day of life. This quick process of elimination leaves infection as the probable cause of the infant's thrombocytopenia. Early-onset bacterial sepsis was appropriately considered in this case, and the infant underwent a workup for sepsis and received broad-spectrum antibiotics. However, there were no risk factors for neonatal sepsis, such as maternal fever, chorioamnionitis, or premature labor. The normal white-cell count and the relatively benign course of illness make this diagnosis even less likely.
The main clinical features in this case are most consistent with an infection acquired in utero. Table 3 lists the organisms causing intrauterine infections that might have some or all of the principal features seen in this case — namely, thrombocytopenia, hepatosplenomegaly, and intrauterine growth retardation.1,2,3,4,5,6 Table 3 also includes my best estimate of the current overall incidence of each of these infections and the likelihood that a child will have symptoms and signs at birth. CMV is the most common agent in the differential diagnosis and thus must be considered in any infant who is thought to have an intrauterine infection. Congenital toxoplasmosis is the infection most likely to be confused with CMV infection, but population-based screening in the United States indicates that toxoplasmosis infects newborns much less often than CMV infection. There are also distinguishing clinical features; the rash observed in infants with congenital toxoplasmosis is usually maculopapular rather than petechial, and infants with toxoplasmosis have chorioretinitis more often than those with congenital CMV infection.
Table 3. Incidence of Selected Intrauterine Infections (per 100,000 Births) in the United States.
Vertically transmitted infection with the human immunodeficiency virus (HIV) has dropped from a peak of approximately 1600 cases in 1992 to fewer than 200 cases in 2000. In the United States, approximately 30 percent of HIV-infected infants who are not being breast-fed acquired the infection during gestation, but they usually have no symptoms at birth. The rare newborns with symptomatic HIV infection have had intrauterine growth retardation, hepatosplenomegaly, pancytopenia, diffuse leukoencephalopathy, and early-onset Pneumocystis carinii pneumonia and have died early in life.7,8
In congenital rubella, the rash tends to be more purpuric than petechial, and cataracts and congenital heart disease are common.9 Neither of the latter findings is present in this patient. Congenital syphilis, which is rapidly declining in incidence in the United States, is strongly associated with drug use by the mother. Infants with congenital syphilis have a scaly, copper-colored, macular rash in the first weeks of life, as well as mucous-membrane lesions and evidence of osteochondritis. Intrauterine infections can occur with either herpes simplex virus or varicella–zoster virus, although the former is far more likely to cause postnatal disease after intrapartum exposure, and intrauterine infection with either virus is rare. In most reported cases, congenital infection with herpes simplex virus or varicella–zoster virus has resembled congenital CMV infection, but these cases have also involved unique vesicular skin lesions or cutaneous scarring and, in congenital varicella, hypoplasia of the limbs.10,11
CMV is a ubiquitous human herpesvirus that is the most common cause of intrauterine infection, affecting approximately 1 percent of all newborn infants. The fetus may become infected if a woman has a primary infection during pregnancy or if she has reactivation of a latent infection that was acquired before pregnancy. Although as many as 2 percent of women who are seropositive for CMV before pregnancy will deliver an infected infant, it is very rare for such infants to have any clinical symptoms.12,13 In contrast, about 15 percent of infants born to women with primary infection have clinical disease that ranges from mild to severe.14,15,16
Most primary CMV infections in pregnancy occur in the early child-bearing years, when the rate of sexual transmission is high. The mother of this infant was 32 years old, well beyond the age range normally associated with primary CMV infection. It is interesting to speculate that during pregnancy, this previously seronegative woman may have acquired the infection from an older child who had acquired the infection in a day-care center. The rate of CMV seroconversion in women with at least one child at home is about twice as high as it is in women without children in the household.17 Furthermore, horizontal transmission is responsible for the high prevalence of infection among toddlers and preschool children who attend day-care centers.18
To summarize, the clinical and laboratory features suggest that this infant has acquired a vertically transmitted infection in utero. Consideration of both the epidemiologic and clinical data makes CMV infection the likely cause, but I cannot rule out toxoplasmosis, rubella, or infection with herpes simplex virus, varicella–zoster virus, or even HIV from the available information. I would approach the diagnosis in two steps, looking first for evidence of CMV infection and then testing for the other agents only if CMV infection appears unlikely. Isolation of CMV in cell culture remains the diagnostic standard. The virus can be isolated from several sources, but urine is the best specimen because of the high titer of virus that is invariably present. Many laboratories use one or more techniques to enhance or speed the identification of virus in cell culture; one such technique is the use of shell vials and monoclonal antibodies directed against early CMV antigens.
Dr. Nancy Lee Harris: Dr. Catlin, you cared for this patient in the newborn nursery. Would you give us your impressions before the diagnostic procedure?
Dr. Elizabeth A. Catlin (Pediatrics): My colleagues and I considered the causes of neonatal thrombocytopenia that Dr. Modlin has discussed and focused primarily on infection. Congenital CMV infection seemed most likely, given the combination of findings.
Clinical Diagnosis
Congenital cytomegalovirus infection.
Dr. John F. Modlin's Diagnosis
Congenital cytomegalovirus infection or another infection vertically transmitted in utero.
Diagnostic Discussion
Dr. Harris: The diagnostic procedures were both imaging studies and a laboratory test.
Dr. P. Ellen Grant: Cranial ultrasonography was performed on the infant's first day of life. A coronal image at the level of the third ventricle showed cystic areas in the region of the germinal matrix at the caudothalamic groove. In a more posterior region of the brain, at the level of the atria of the lateral ventricle, there were multiple periventricular foci of echogenicity, which were thought to represent calcifications. On cranial computed tomographic scanning, the echogenic foci were confirmed to be areas of calcification; many areas of calcification can be seen in a periventricular location (Figure 2A). The distribution of these lesions is typical of CMV infection, which has a predilection to involve the rapidly multiplying cells of the germinal matrix. On magnetic resonance imaging, an abnormal gyral folding pattern (affecting the right hemisphere more than the left) is visible, and in the affected areas, the junction between the gray matter and the white matter is irregular (Figure 2B) — these findings are consistent with the presence of diffuse polymicrogyria. In the occipital regions, small periventricular pseudocysts are also evident. The cerebellum is hypoplastic.
View larger version (45K):
[in this window]
[in a new window]
Figure 2. Cranial Imaging Studies.
An axial CT image of the cranium, obtained without the use of contrast material (Panel A), shows multiple punctate, periventricular foci of calcification (arrowheads). An axial image from a T2-weighted MRI study (Panel B) shows multiple regions of abnormal gyral folding (arrowheads), a finding consistent with the presence of polymicrogyria. The punctate foci of decreased T2 signal (arrows) correspond to calcifications, which are better seen on the CT scan. The white matter has an abnormally increased T2 signal, and the ventricles are enlarged.
The findings on imaging — calcifications that are predominantly periventricular, periventricular pseudocysts, polymicrogyria, and cerebellar hypoplasia — are almost pathognomonic for CMV infection. In addition, they tend to rule out toxoplasmosis, which is associated with enlarged ventricles without cortical malformations, as well as other congenital infections.
Dr. Robert S. Makar: The laboratory test used in this case was a shell-vial assay for CMV. The shell-vial assay is a variant of routine culture methods used to detect CMV in clinical specimens. In routine culture, CMV infection of cultured fibroblasts results in a characteristic cytopathic effect. Although the appearance of the cytopathic effect is a sensitive marker of viral infection, it can take several days to occur, depending on the viral titer in the clinical specimen. In contrast, with the shell-vial assay, virus can be detected within 24 hours after inoculation.19 In brief, glass coverslips bearing the cultured cells are placed in vials containing culture medium. The vials are inoculated with the specimen and then centrifuged at low speed to facilitate viral adsorption.20 Viral infection is then detected by indirect immunofluorescence for immediate-early antigens in the nuclei of the cultured cells. This patient's urine was floridly positive for CMV according to the shell-vial assay (Figure 3).
View larger version (47K):
[in this window]
[in a new window]
Figure 3. Shell-Vial Assay for Cytomegalovirus (CMV) (Immunofluorescence Stain, x400).
Fibroblasts inoculated with the patient's urine show apple-green nuclear staining with antibody to CMV immediate-early antigen, indicating CMV infection. The assay was performed with reagents obtained from Chemicon International.
Many tests are available for the diagnosis of CMV infection, but not all of them are reliable for the diagnosis of congenital infection. Detection of CMV antigenemia is a sensitive test for CMV infection in immunocompromised adults but has not been validated as a test for congenital CMV. Serologic tests for fetal IgG and IgM antibodies against CMV are difficult to interpret. Since IgG antibodies are passively transferred from mother to fetus, a positive anti-CMV IgG titer in fetal blood is not meaningful. Anti-CMV IgM antibodies do not cross the placenta, and their presence in cord blood suggests congenital infection. However, the sensitivity and specificity of currently available tests for IgM antibodies do not yet match those of viral-culture methods or polymerase-chain-reaction (PCR) assays for viral genetic material.1 Thus, the diagnosis of congenital CMV infection hinges on the detection of virus by one of the latter two methods. Clinical specimens should be obtained within two weeks after birth to allow congenital and perinatal infections to be distinguished from one another.
Prenatal diagnosis of congenital CMV infection can be offered to women in whom seroconversion occurs during pregnancy. The isolation of virus or viral DNA from amniotic fluid is the most reliable measure of congenital infection.1 However, a negative result may not rule out infection, even when the sample of amniotic fluid is obtained after 20 weeks of gestation,21 and a positive result does not necessarily correlate with symptomatic infection.22 A recent study suggests that a high CMV load in the amniotic fluid on quantitative PCR is correlated with symptomatic infection23 and thus may be useful as a prognostic tool in congenital CMV infection.
Dr. Harris: As is the routine when an infant is born ill, the placenta was examined in this case, and I would like to ask Dr. Drucilla Roberts to describe the findings.
Dr. Drucilla J. Roberts: The placenta was a small, singleton placenta; it weighed 310 g (below the 10th percentile for 39 weeks' gestation) and was discolored (greenish-brown) by meconium pigment. At least 50 percent of the villi were avascular, with open maternal vascular spaces (Figure 4). This finding represents vascular compromise from the fetal (not maternal) circulation to the placenta.24
View larger version (51K):
[in this window]
[in a new window]
Figure 4. Histologic Section of the Placenta (Hematoxylin and Eosin, x250).
Avascular villi (arrow), with open maternal vascular spaces (arrowhead), are visible.
The pathological differential diagnosis of avascular villi (Table 4) includes chronic villitis, either active or healed.25 Chronic villitis, which is seen in up to 10 percent of all placentas examined histologically, is characterized by a maternal inflammatory infiltrate, typically mononuclear, in the villi. Most cases are thought to be due to a maternal factor (perhaps an immune response to the fetal allograft). A small number of cases are due to transplacental infection, with CMV being the most common agent.
Table 4. Pathological Differential Diagnosis of Avascular Villi.
The histopathological features of CMV placentitis include lymphoplasmacytic villitis, sclerosis of the villous capillaries, chorionic vessel thromboses, necrotizing villitis, hemosiderin deposition in the villous stroma, and immature nucleated fetal red cells in the blood vessels and viral inclusions (seen in approximately 10 percent of cases).26 In the infant in the current case, there was no active chronic villitis, none of the features of an active CMV placentitis were present, and immunohistochemical stains for CMV antigen were negative.27
Infants with a remote transplacental CMV infection often have nonspecific findings of villous sclerosis and chorionic vascular thromboses, and the weight of their placentas may be below the 10th percentile. The placental pathological findings in this case are consistent with a CMV villitis that developed at least two weeks before birth and possibly earlier and that has scarred, leaving the avascular sclerotic villi.
Dr. Harris: Since we assumed that the diagnosis in this case would not be a problem for Dr. Modlin, I asked him to tell me his diagnosis before the conference and then invited him to discuss current issues in the management of congenital CMV infection.
Discussion of Management
Dr. Modlin: The case under discussion is representative of the approximately 10 percent of CMV-infected newborns who have clinical evidence of disease in the neonatal period. The severity of the infection appears to be related to the age of the fetus at the time of the infection: those infected during the first trimester have relatively severe consequences, whereas those infected during the third trimester may have no symptoms. The spectrum of signs and symptoms includes premature delivery, intrauterine growth retardation, microcephaly, jaundice, petechiae, hepatosplenomegaly, thrombocytopenia, indirect and direct hyperbilirubinemia, and other signs of mild hepatitis (Table 5).
Table 5. Selected Clinical and Laboratory Findings in 106 Infants with Symptomatic Intrauterine Congenital Cytomegalovirus Infection in the Neonatal Period.
The mortality rate is approximately 20 percent. For those who survive, the hematologic abnormalities, hepatitis, and other manifestations not involving the central nervous system resolve within weeks to months after birth, despite ongoing shedding of the virus, which persists for months to years after birth.28 However, about 60 percent of these infants have sensorineural hearing deficits, and in about 70 percent microcephaly, seizures, motor abnormalities, developmental delay, or other cognitive impairments occur.29 Overall, 90 percent of the surviving infants will have either a sensory deficit or cognitive impairment.
Although the initial insult occurs in utero, the developing central nervous system remains vulnerable to damage from persistent viral replication after birth, and thus effective antiviral therapy given after birth may reduce the severity of the neurologic damage and improve the long-term outcome.30,31 The first opportunity to test this hypothesis came with the development of ganciclovir, a derivative of acyclovir, which was the first antiviral agent capable of inhibiting CMV replication at clinically attainable concentrations. The Collaborative Antiviral Study Group of the National Institute of Allergy and Infectious Diseases recently completed a phase 3 trial of intravenous ganciclovir for symptomatic congenital CMV disease in infants.32 This challenging trial required the parents of infants with a devastating prognosis to accept random assignment to treatment with ganciclovir or no treatment and required the placement of a central venous catheter and twice-daily intravenous treatment. The infants who were randomly assigned to a six-week course of intravenous ganciclovir had significantly better hearing and more rapid resolution of hepatitis than the infants who were not treated.
These unequivocal results provide proof of concept and allow us to proceed to studies designed to optimize antiviral therapy for CMV-infected newborns. A planned Collaborative Antiviral Study Group trial will evaluate longer-term treatment with valganciclovir, a recently licensed prodrug that reaches serum concentrations similar to those of ganciclovir when given orally. If this study shows that valganciclovir is effective in further reducing the morbidity associated with symptomatic congenital CMV infection, then it follows that treatment of the 90 percent of infected infants who have no symptoms at birth but who have a lower but well-documented risk of hearing loss than those with signs of infection at birth will be the target of further antiviral research.1 In turn, this would raise a brand-new issue for those who study the feasibility and outcomes of newborn screening and perform cost–benefit analyses. At this moment, the future for the diagnosis and treatment of congenital CMV infections looks very promising.
Dr. Harris: Dr. Walsh will discuss the treatment decision that was made in the current case.
Dr. Walsh: We reviewed the published phase 2 data on the use of intravenous ganciclovir for congenital CMV infection33 and contacted a colleague at the University of Alabama at Birmingham, who shared with us preliminary data from the phase 3 trial of ganciclovir.29 The data were particularly encouraging with respect to the stabilization of hearing loss. We then discussed treatment options with the parents of the infant in this case, and they opted to have their infant receive intravenous ganciclovir for six weeks. Therapy was completed without serious complications.
Dr. Harris: Dr. Casavant, you are this patient's primary care physician and have been working with the family during the administration of treatment at home. Would you discuss some of the issues and tell us how the patient is doing now?
Dr. David W. Casavant (Pediatrics): After the diagnosis was established, further evaluation showed mild CMV-associated chorioretinitis and profound hearing loss in the left ear. The ganciclovir treatment required placement of a central venous catheter and twice-weekly testing of blood samples to monitor the complete blood count for evidence of neutropenia or anemia, since ganciclovir is toxic to the bone marrow. One of the parents' chief problems during the first months after the infant's birth was the fear of other family members that they or their children might be infected by the infant. We tried to assure them that CMV infection is quite common and is not associated with problems in immunocompetent persons, when acquired after the neonatal period.
Although the literature forecasts a rather bleak picture for the patient's development, he has done remarkably well. At his most recent routine visit, he was approximately 22 weeks old and had only mild left-sided weakness and some resolving torticollis.
Dr. Harris: This patient was evaluated and followed by Dr. Krishnamoorthy. Dr. Krishnamoorthy, would you review the neurologic complications of congenital CMV infection and tell us about this patient's neurologic status and prognosis?
Dr. Kalpathy S. Krishnamoorthy: Neonates with CMV infection can be divided into three prognostic groups. Up to 95 percent of those with overt manifestations in the central nervous system (e.g., microcephaly, cerebral calcification, or chorioretinitis) have major neurodevelopmental sequelae; those with only systemic manifestations (e.g., jaundice, petechiae, or hepatosplenomegaly) are still at risk but have a slightly better prognosis; and those with neither central nervous system nor systemic manifestations have the best prognosis. However, even infants with no symptoms are at risk for developmental delay, microcephaly, motor deficits, and (most commonly) sensorineural hearing loss, which may not become apparent until late infancy or early childhood.34 An important clinical point is that congenital CMV infection should be included in the differential diagnosis of developmental delay associated with microcephaly and sensorineural hearing loss during infancy, even in the absence of neonatal manifestations of CMV infection.
Microcephaly is the most specific predictor of mental retardation and major motor disability. In a recent study,35 the combination of microcephaly and abnormal findings on CT imaging carried the worst prognosis (mean IQ score, <50; major motor deficit in 75 percent of the patients); a normal head circumference and normal CT findings were associated with a good prognosis (mean IQ score, >90; no major motor deficit); and a normal head circumference and abnormal CT findings were associated with an intermediate prognosis (mean IQ score, 70 to 80; major motor deficit in 37 percent).
In view of the abnormalities seen on CT scanning in this infant, he falls into the intermediate prognostic group. We have seen him twice in follow-up, most recently when he was 14 weeks of age. His head circumference has stayed at the 25th percentile, which is in line with his overall size. He remains visually alert and sociable and has a good smile. Assessment of muscle tone shows diffuse, mild hypertonia that is manifested as prominent clenching of the fists and excessive arching of the back. Left-sided sensorineural hearing loss persists, but the ophthalmologic findings remain normal. His prognosis remains uncertain.
Dr. Grant: The presence of polymicrogyria on the imaging studies suggests that the major injury to the fetal brain occurred somewhere between 20 and 25 weeks' gestational age. Would it have been possible to treat the mother when she seroconverted?
Dr. Modlin: The usual problem is detecting infection in the pregnant woman, because the majority of these infections are completely silent. Unfortunately, it is not clear that there is an effective and safe prenatal treatment for fetal CMV infection.
Dr. Casavant: Because of the mother's equivocal IgM response to CMV in the presence of IgG antibodies, the possibility of recent infection was discussed with her early in the pregnancy. However, there are no guidelines for treatment of CMV infection during pregnancy.
Pathological Diagnosis
Congenital cytomegalovirus infection.
We are indebted to Dr. Elizabeth Catlin for assistance in preparing the case abstract and to Dr. Mark Pasternack for assistance in organizing the conference.
Source Information
From the Departments of Pediatrics and Medicine, Dartmouth–Hitchcock Medical Center and Dartmouth Medical School, Lebanon, N.H. (J.F.M.); the Departments of Radiology (P.E.G.), Pathology (R.S.M., D.J.R.), and Pediatrics (K.S.K.), Massachusetts General Hospital and Harvard Medical School.
References
Spagno S. Cytomegaloviruses. In: Remington JS, Klein JO, eds. Infectious diseases of the fetus and newborn infant. 5th ed. Philadelphia: W.B. Saunders, 2001:389-424.
Weller TH, Hanshaw JB. Virologic and clinical observations on cytomegalic inclusion disease. N Engl J Med 1962;266:1233-1244.[ISI]
Guerina NG, Hsu H-W, Meissner HC, et al. Neonatal serologic screening and early treatment for congenital Toxoplasma gondii infection. N Engl J Med 1994;330:1858-1863.[Abstract/Full Text]
Eberhardt MS, Ingram DD, Makuc DM, et al. Urban and rural health chartbook. Health, United States, 2001. Hyattsville, Md.: National Center for Health Statistics, 2001.
Congenital syphilis -- United States, 2000. MMWR Morb Mortal Wkly Rep 2001;50:573-577.[Medline]
Reyes MP, Hunt N, Ostrea EM Jr, George D. Maternal/congenital syphilis in a large tertiary-care urban hospital. Clin Infect Dis 1993;17:1041-1046.[ISI][Medline]
Millard DD, Chadwick EG, Yogev R, Modlin JF. Zidovudine treatment of an infant with congenital human immunodeficiency virus infection. Pediatr Infect Dis J 1990;9:929-931.[ISI][Medline]
Rudin C, Meier D, Pavic N, et al. Intrauterine onset of symptomatic human immunodeficiency virus disease. Pediatr Infect Dis J 1993;12:411-414.[ISI][Medline]
Cooper LZ, Green RH, Krugman S, Giles JP, Mirick GS. Neonatal thrombocytopenic purpura and other manifestations of rubella contracted in utero. Am J Dis Child 1965;110:416-427.[ISI][Medline]
Hutto C, Arvin A, Jacobs R, et al. Intrauterine herpes simplex virus infections. J Pediatr 1987;110:97-101.[ISI][Medline]
Alkalay AL, Pomerance JJ, Rimoin DL. Fetal varicella syndrome. J Pediatr 1987;111:320-323.[ISI][Medline]
Stagno S, Reynolds DW, Huang E-S, Thames SD, Smith RJ, Alford CA Jr. Congenital cytomegalovirus infection: occurrence in an immune population. N Engl J Med 1977;296:1254-1258.[Abstract]
Stagno S, Pass RF, Dworsky ME, Alford CA Jr. Maternal cytomegalovirus infection and perinatal transmission. Clin Obstet Gynecol 1982;25:563-576.[Medline]
Stagno S, Pass RF, Cloud G, et al. Primary cytomegalovirus infection in pregnancy: incidence, transmission to fetus, and clinical outcome. JAMA 1986;256:1904-1908.[Abstract]
Boppana SB, Rivera LB, Fowler KB, Mach M, Britt WJ. Intrauterine transmission of cytomegalovirus to infants of women with preconceptional immunity. N Engl J Med 2001;344:1366-1371.[Abstract/Full Text]
Fowler KB, Stagno S, Pass RF, Britt WJ, Boll TJ, Alford CA. The outcome of congenital cytomegalovirus infection in relation to maternal antibody status. N Engl J Med 1992;326:663-667.[Abstract]
Dworsky ME, Welch K, Cassady G, Stagno S. Occupational risk for primary cytomegalovirus infection among pediatric health-care workers. N Engl J Med 1983;309:950-953.[Abstract]
Adler SP. Cytomegalovirus transmission among children in daycare, their mothers and caretakers. Pediatr Infect Dis J 1988;7:279-285.[ISI][Medline]
Hodinka RL, Friedman HM. Human cytomegalovirus. In: Murray PR, Baron EJ, Pfaller MA, Tenover FC, Yolken RH, eds. Manual of clinical microbiology. 6th ed. Washington, D.C.: ASM Press, 1995:884-94.
Gleaves CA, Smith TF, Shuster EA, Pearson GR. Rapid detection of cytomegalovirus in MRC-5 cells inoculated with urine specimens by using low-speed centrifugation and monoclonal antibody to an early antigen. J Clin Microbiol 1984;19:917-919.[ISI][Medline]
Azam A, Vial Y, Fawer CL, Zufferey J, Hohlfeld P. Prenatal diagnosis of congenital cytomegalovirus infection. Obstet Gynecol 2001;97:443-448.[CrossRef][ISI][Medline]
Lazzarotto T, Guerra B, Spezzacatena P, et al. Prenatal diagnosis of congenital cytomegalovirus infection. J Clin Microbiol 1998;36:3540-3544.[Abstract/Full Text]
Guerra B, Lazzarotto T, Quarta S, et al. Prenatal diagnosis of symptomatic congenital cytomegalovirus infection. Am J Obstet Gynecol 2000;183:76-82.[ISI][Medline]
Roberts D, Schwartz RS. Clotting and hemorrhage in the placenta -- a delicate balance. N Engl J Med 2002;347:57-59.[Full Text]
Gersell DJ. Chronic villitis, chronic chorioamnionitis, and maternal floor infarction. Semin Diagn Pathol 1993;10:251-266.[ISI][Medline]
Benirschke K, Mendoza GR, Bazeley PL. Placental and fetal manifestations of cytomegalovirus infection. Virchows Arch B Cell Pathol 1974;16:121-139.
Muhlemann K, Miller RK, Metlay L, Menegus MA. Cytomegalovirus infection of the human placenta: an immunocytochemical study. Hum Pathol 1992;23:1234-1237.[ISI][Medline]
Stagno S, Pass R, Dworsky ME, Alford CA. Congenital and perinatal cytomegalovirus infections. Semin Perinatol 1983;7:31-42.[ISI][Medline]
Kimberlin DW, Lin CY, Sanchez P, et al. Ganciclovir (GCV) treatment of symptomatic congenital cytomegalovirus (CMV) infections: results of a phase III randomized trial. Presented at the 40th Interscience Conference on Antimicrobial Agents and Chemotherapy, Toronto, September 17–20, 2000. abstract.
Kimberlin DW. Antiviral therapy for cytomegalovirus infections in pediatric patients. Semin Pediatr Infect Dis 2002;13:22-30.[CrossRef][Medline]
Whitley RJ, Kimberlin DW. Treatment of viral infections during pregnancy and the neonatal period. Clin Perinatol 1997;24:267-283.[ISI][Medline]
Kimberlin DW, Lin C-Y, Sanchez PJ, et al. Effect of ganciclovir therapy on hearing in symptomatic congenital cytomegalovirus disease involving the central nervous system: a randomized, controlled trial. J Pediatr (in press).
Whitley RJ, Cloud G, Gruber W, et al. Ganciclovir treatment of symptomatic congenital cytomegalovirus infection: results of a phase II study. J Infect Dis 1997;175:1080-1086.[ISI][Medline]
Fowler KB, McCollister FP, Dahle AJ, Boppana S, Britt WJ, Pass RF. Progressive and fluctuating sensorineural hearing loss in children with asymptomatic congenital cytomegalovirus infection. J Pediatr 1997;130:624-630.[ISI][Medline]
Noyola DE, Demmler GJ, Nelson CT, et al. Early predictors of neurodevelopmental outcome in symptomatic congenital cytomegalovirus infection. J Pediatr 2001;138:325-331.[CrossRef][ISI][Medline]
"Even though SV-40 was being screened out, scientists such as John Martin, a professor of pathology at the University of Southern California, warned that other monkey viruses could be dangerous. But government officials rebuffed Martin's attempt to research those risks back in 1978 and again in 1995 when he was denied federal funding and vaccine samples he needed to investigate the effects of simian cytomegalovirus (SCMV), an organism that his studies indicate causes neurological disorders in the human brain."--Money Magazine
http://members.jorsm.com/~binstock/fs-hhv6.htm
1 MMR/HHV-6: general considerations
>>> Posting number 25001,
dated 2 Oct 1997 14:37:47
Here are some thoughts about MMR and HHV-6. We must keep in mind that each child is different and that the timing during which a child might have acquired HHV-6 will differ from person to person. Therefore, the following comments should be taken as a general sketch, a starting point in trying to understand each child's specific case. We must also keep in mind that, in many individuals, there may be more than one virus, bacteria, and/or fungus present; and this kind of inter-individual variation is likely to be seen as differences in each child's specific traits and medical history. So, here are some thoughts centered upon MMR and HHV- 6.
1. Measles and measles vaccinations induce immunospression. This is well known, well documented; and a primary researcher in this is Diane E. Griffin of JohnsHopkins. (Cites will be in subseqeunt post).
2. HHV-6 is ubiquitous, many kids have it and handle it quite OK. However, HHV-6 is also known to induce high fever and/or seizures in a goodly number of kids. The healthier a given child's immune system, the likelier that HHV-6 will not cause problems to that child.
3. At least hypothetically, the immunosuppression that accompanies measles vaccination would allow HHV-6 to blossom more fully within the child. What might be seen is roseola (aka exanthema subitum) and/or fevers and/or some mild or not so mild febrile convulsions. (some HHV-6 cites will be posted separately too).
4. HHV-6 is also known to be able to produce its own immunosuppression, and can even find its way into bone marrow. In some children, the HHV-6 immunosuppression would become additive with the immunosuppression already induced by the measles component of the MMR vaccination.
5. Giving MMR prior to the age of 12 months would seem to be a way to ensure aprolonged Transient Hypogammaglobulinemia of Infancy (pTHI), thereby inducing another kind of double immunosuppression -- that from the infant's normal THI plus that from measles-vaccination immunosuppression.
6. If a pregnant woman were to receive a measles vaccination, then her measles-related immunosuppression would increase the likelihood that other viruses, bacteria, and/or fungi would gain a foothold or (if present and normally immunosuppressed) to blossom in ways affecting fetal development.
7. The work of Tasnee Chonmaitree and colleagues has demonstrated that many cases of recurrent otitis media (rOM) are viral in origin. In a study of 271 kids with rOM, 10 percent were found to have cytomegalovirus and/or herpes simplex virus in middle ear effusion (CMV, HSV, MEM). Her studies prove that, in some kids, heavy duty viruses can be present at an early age, even if the only symptom is rOM.
8. HHV-6, CMV, and Epstein-Barr virus (EBV) are known to be able to induce immunosuppression. When Drs. Baker and Martin find CMV in peripheral blood, that is a very important finding. Treating the CMV and reducing it or eliminating it can only help the child -- even if he or she has other viruses in the CNS, viruses that may not be detectable by peripheral measures or even via viral culture of CSF.
9. If an infant has any of these viruses (eg, HHV-6, CMV, or EBV) in his or her system when the MMR is given, then (due to the immunosuppressivity of the measles component) that child would seem at risk for any of the three immunosuppressive viruses to become more entrenched and active.
10. HSV is a very special virus. It is present in some kids with recurrent otitis media (rOM), yet may remain within the CNS with *no* exterior symptoms one the otitis has subsided. Depending upon its route of entry (eg, oral/gastrointestinal, nasal-cativy, scraped skin, etc), HSV will travel to various parts of the peripheral and central nervous systems. Once there, if a child is immunocompetent, the virus may remain latent and, while latent, may induce no neuronal death.
11. If HSV is latently present in CNS neurons when the MMR is given, two effects are likely: (i) the measles-induced immunosupression may allow some of the latent HSV to become re-activated, and (ii) the MMR's induction of interferon gamma (1) ought lead to MHC-I presentation of viral particles upon the surface of neurons, which would then be killed by the person's own immune surveillance processes. Importantly, HSV is capable of migrating to neural substrates that have been identified in autism (eg, cerebellum and temporal lobe) and/or that participate in autistic traits -- eg, neuronal regions subserving language, emotions, sensory sensitivities, and direct eye-contact.
.....Closing Comments.....
Each child is very different; each child's medical history prior to, during, and subsequent to the MMR is very different and ought be considered as the tapestry in which the MMR and HHV-6 occurred.
Several parental anecdotes have mentioned the temporal sequence MMR followed by signs of HHV-6. This is an extremely important relationship, and possible causal links were outlined in the first portion of this document. However, each parent would be well served to look for additional clues prior to and subsequent to the vaccination. Such introspection may generate additional clues instructive regarding the child's specific pathogenesis into autism and, most importantly, may provide
clues towards designing the most effective treatments.
In other words, the link "MMR and HHV-6" is important, but each child's medical history may have some additional clues that can be considered --eg, familial infections such as mononucleosis or herpes or? eg, gastrointestinal problems in the child and/or in other members of the family or ? eg, other?
These developments are very exciting and are occurring because of each person's committment to ask questions and to share. From the pioneers such as Rimland, Baker, Pangborn, Martin and others, to the parents and a few researchers, and a growing number of parents-as-researchers, might we say, Progress is being made and shall continue!
1) Pabst HF et al. Kinetics of immunologic responses after primary MMR vaccination. Vaccine. 15(1):10-4, 1997 Jan. "To study the kinetics of humoral as well as cellular immunity to measles and to test for associated immunosuppression 124 12 month old children were studied twice, before routine MMR and either 14, 22, 30, or 38 days after vaccination...Interferon-gamma was the principal cytokine produced after primary measles immunization..."
2 MMR/HHV-6: immune suppression by measles virus/vaccine
>>> Posting number 25023,
dated 2 Oct 1997 20:15:14
Measles virus can induce immune suppression, by vaccinations and/or infection. The first seven citations are by DE Griffin and colleagues. Cites 8 thru 10 are by other groups researching immunosuppression caused by measles virus, whether the "wild-type" or the type found in certain vaccines.
<1> Karp CL. Wysocka M. Wahl LM. Ahearn JM. Cuomo PJ. Sherry B. Trinchieri G. Griffin DE.
Mechanism of suppression of cell-mediated immunity by measles virus Science. 273(5272):228-31, 1996 Jul 12.
<2> Hussey GD et al.
The effect of Edmonston-Zagreb and Schwarz measles vaccines on immune response in infants.
Journal of Infectious Diseases. 173(6):1320-6, 1996 Jun.
<3> Auwaerter PG et al Changes within T cell receptor V beta subsets in infants following
measles vaccination. Clinical Immunology & Immunopathology. 79(2):163-70, 1996 May.
<4> Griffin DE. Immune responses during measles virus infection. Current Topics in Microbiology & Immunology. 191:117-34, 1995.
<5> Ward BJ. Griffin DE.
Changes in cytokine production after measles virus vaccination: predominant production of IL-4 suggests induction of a Th2 response. Clinical Immunology & Immunopathology. 67(2):171-7, 1993 May.
<6> Wu VH. McFarland H. Mayo K. Hanger L. Griffin DE. Dhib-Jalbut S.
Measles virus-specific cellular immunity in patients with vaccine failure.
Journal of Clinical Microbiology. 31(1):118-22, 1993 Jan.
<7> Griffin DE et al
In vitro studies of the role of monocytes in the immunosuppression associated with natural measles virus infections. Clinical Immunology & Immunopathology. 45(3):375-83, 1987 Dec.
<8> Schnorr JJ et al.
Induction of maturation of human blood dendritic cell precursors by measles virus [vaccine & wild type] is associated with immunosuppression.
Proc of the National Acad of Sciences USA 94(10):5326-31 1997. As well as inducing a protective immune response against reinfection, acutemeasles is associated with a marked suppression of immune functions against superinfecting agents and recall antigens, and this association is the major cause of the current high morbidity and mortality rate associated with measles virus (MV) infections. Dendritic cells (DCs) are antigen-presenting cells crucially involved
in the initiation of primary and secondary immune responses, so we set out to define the interaction of MV with these cells. We found that both mature and precursor human DCs generated from peripheral blood monocytic cells express the major MV protein receptor CD46 and are highly susceptible to infection with both MV vaccine (ED) and wild-type (WTF) strains, albeit with different kinetics. Except for the down-regulation of CD46, the expression pattern of functionally important surface antigens on mature DCs was not markedly altered after MV infection. However,precursor DCs up-regulated HLA-DR, CD83, and CD86 within 24 h of WTF infection and 72 h after ED infection, indicating their functional maturation. In addition, interleukin 12 synthesis was markedly enhanced after both ED and WTF infection in DCs. On the other hand, MV-infected DCs strongly interfered with mitogen-dependent proliferation of freshly isolated peripheral blood lymphocytes in
vitro. These data indicate that the differentiation of effector functions of DCs is not impaired but
rather is stimulated by MV infection. Yet, mature, activated DCs expressing MV surface antigens do give a negative signal to inhibit lymphocyte proliferation and thus contribute to MV-induced immunosuppression.
<9> Aaby P.
Assumptions and contradictions in measles and measles immunization research: is measles good for something?. Social Science & Medicine. 41(5):673-86, 1995 Sep. Measles infection, the major cause of childhood mortality among infections preventable by immunization, has been considered to kill mainly young and malnourished children. Assuming that mainly 'weak' children are saved by immunizations, it has been speculated that the impact on survival of immunization is likely to be limited because the malnourished children are more prone to die of other infections. However, recent studies from developing countries have suggested that host factors may not be the most important determinants of acute and long-term mortality after measles infection. Instead, it was found that infection contracted after exposure at home infection contracted from someone outside the home.
Furthermore, measles is particularly severe if contracted from someone of the opposite sex. Hence transmission factors, in particularly intensity of exposure and cross-sex transmission, may be more important determinants of measles mortality than the determinants of measles mortality than the host factors usually emphasized. Consistent with these observations and in contrast to assumptions
about 'weak' children dying, immunization is associated with a major reduction in mortality.Since measles immunization is associated with a 30% reduction in mortality or more, the impact is much larger than should be expected from the proportion of all deaths attributed to measles. It has therefore been suggested that measles immunization may prevent the persistent immunosuppression and delayed mortality assumed to beassociated with measles. However, several observations contradict the common understanding that the function of measles immunization is only to prevent the acute and long-term mortality associated with measles infection. Recently, the high-titre measles immunization recommended by WHO was found to be associated
with reduced survival for female recipients compared with girls who have received the standard low-dose measles vaccine, and this difference in survival was not due to suboptimal protection against measles infection. Contrary to usual assumptions. against measles infection. Contrary to usual assumptions, standard low-dose measles vaccine reduces mortality even more when given before 9 months of age, the age currently recommended by WHO. The beneficial impact of standard vaccine is apparently temporary, lasting 1 to 2 years, whereas it should increase with the age of the child. The beneficial effect seems to be particularly strong for girls. The most likely interpretation of these observations, is that standard low-dose measles vaccine has a non-specific beneficial effect. Contrary to current assumptions, children who survive the acute phase of measles infection may have a survival advantage compared with unimmunized, uninfected children...
<10> Smedman L et al.
Immunosuppression after measles vaccination.
Acta Paediatrica. 83(2):164-8, 1994 Feb.
The influence of conventional live attenuated measles vaccine on cellular immune responsiveness was investigated in Sweden and Guinea-Bissau. Sixteen children in a residential area in Bissau and 16 living in southern Stockholm were examined before and 8-10 days after vaccination... These observations may be relevant to the increased mortality found in children immunized with high-titre
measles vaccines, as compared to controls, in recent studies...
J Autism Dev Disord. 2004 Oct;34(5):583-6.
Brief report: autistic disorder in three children with cytomegalovirus infection.
Sweeten TL, Posey DJ, McDougle CJ.
Department of Psychiatry, Indiana University School of Medicine, Indianapolis, IN 46202-4800, USA.
Previous research has identified a relationship between autistic disorder (autism) and specific congenital infections. Three cases of congenital or perinatal cytomegalovirus (CMV) infection occurring in association with autism are described. Hypothetical mechanisms relating congenital infection, such as CMV, to the development of autism are discussed. A better understanding of the immunologic response to certain congenital infections may provide important information pertaining to the pathophysiology and etiology of autism in vulnerable individuals.
Subject: Cytomegalovirus infection and development of allergic diseases
J Allergy Clin Immunol. 2004 Dec;114(6):1434-40.
Cytomegalovirus infection and development of allergic diseases in early childhood: interaction with EBV infection?
Sidorchuk A, Wickman M, Pershagen G, Lagarde F, Linde A.
Institute of Environmental Medicine, Stockholm, Sweden.
BACKGROUND: Chronic replication of cytomegalovirus and EBV in early life may affect the immune system and play a role in the development of allergy in children. OBJECTIVE: To assess the relation between cytomegalovirus infection and allergic disorders in children, including a possible interaction with EBV infection. METHODS: From a prospective birth cohort study in Stockholm, on factors of importance for development of allergy, 2581 four-year-old children were enrolled. The classification of allergic diseases was based on questionnaire answers and determination of IgE antibodies to common airborne and food allergens. IgG to cytomegalovirus was determined by a commercial ELISA and to EBV by indirect immunofluorescence. RESULTS: A total of 1191 (46%) children were cytomegalovirus-seropositive. There were no significant associations between seropositivity to cytomegalovirus and allergic manifestations, such as bronchial asthma, suspected allergic rhinitis, or atopic dermatitis. Seropositivity to cytomegalovirus alone, ie, without seropositivity to EBV, was related to IgE antibodies to airborne and food allergens (adjusted odds ratio, 1.8; 95% CI, 1.2-2.9). An antagonism between cytomegalovirus and EBV in relation to sensitization to airborne and food allergens was suggested ( P = .05). CONCLUSION: The study does not support the hypothesis that previous cytomegalovirus infection plays an important role in the pathogenesis of bronchial asthma, suspected allergic rhinitis, or atopic dermatitis in children. However, in the absence of EBV infection, cytomegalovirus infection may be related to sensitization to airborne and food allergens.
Lopez-Pison J, Rubio-Rubio R, Urena-Hornos T, Omenaca-Teres M, Sans A, Cabrerizo de Diago R, Pena-Segura JL. Retrospective diagnosis of congenital infection by cytomegalovirus in the case of one infant. Rev Neurol. 2005;40:733-6.
Sweeten TL, Posey DJ, McDougle CJ. Brief report: autistic disorder in three children with cytomegalovirus infection. J Autism Dev Disord. 2004; 34:583-6.
Yamashita Y, Fujimoto C, Nakajima E, Isagai T, Matsuishi T. Possible association between congenital cytomegalovirus infection and autistic disorder. J Autism Dev Disord. 2003;33:455-9.
Ivarsson SA, Bjerre I, Vegfors P, Ahlfors K. Autism as one of several disabilities in two children with congenital cytomegalovirus infection. Neuropediatrics. 1990;21:102-3.
Stubbs EG, Ash E, Williams CP. Autism and congenital cytomegalovirus. J Autism Dev Disord. 1984;14:183-9.
Markowitz PI. Autism in a child with congenital cytomegalovirus infection. J Autism Dev Disord. 1983;13:249-53.
Stubbs EG. Autistic symptoms in a child with congenital cytomegalovirus infection. J Autism Child Schizophr. 1978;8:37-43.
It is also known that up to 20% of cytomegalovirus infected blood samples will test negative using routine antibody based assays (Rahbar AR, Sundqvist VA, Wirgart BZ, Grillner L, Soderberg-Naucler C. Recognition of cytomegalovirus clinical isolates by sera from cytomegalovirus-negative blood donors. Transfusion 2004; 44: 1059-66.) The polymerase chain reaction (PCR) also has limitations, especially in detecting stealth-adapted cytomegaloviruses. By far the best screening test for both regular and stealth-adapted cytomegaloviruses is virus culture. I know from my own experience that the majority of autistic children have evidence of circulating cell damaging viruses (Martin WJ. Stealth virus isolated from an autistic child. J Autism Dev Disord. 1995;25:223-4.)
Parents have a right to expect Public Health authorities to perform appropriate virus cultures on autistic children. As I have said previously “If autism is epidemic, why not look for an infectious cause?”
The Government’s obligation to pursue cytomegalovirus infection is further strengthened by FDA’s own published data that 3 of 8 licensed polio virus vaccines released in the mid 1970’s contain DNA of African green monkey simian cytomegalovirus (Sierra-Honigmann AM, Krause PR. Live oral poliovirus vaccines and simian cytomegalovirus. Biologicals. 2002;30:167-74.) Additional information is available at www.s3support.com Kind regards, W. John Martin, M.D., Ph.D.
Vet Pathol 41:108-115 (2004)
© 2004 American College of Veterinary Pathologists
Cervical and Vaginal Epithelial Neoplasms in Cynomolgus Monkeys C. E. Wood, H. Borgerink, T. C. Register, L. Scott and J. M. Cline
Comparative Medicine Clinical Research Center, Wake Forest University Health Sciences, Winston-Salem, NC
Papillomavirus-associated cervical cancer is the second most common neoplasm in women but has rarely been reported in animals. This report describes cervical and vaginal intraepithelial neoplasms identified in routine histologic specimens obtained from 20 (5.2%) of 385 female cynomolgus macaques (Macaca fascicularis) being used in long-term studies. Lesion incidence was similar in both control and hormonally treated animals (4.7% and 5.5%, respectively). Neoplasms included benign vaginal papillomas, mild to severe intraepithelial dysplasias, and two invasive cervical carcinomas. Common morphologic features included koilocytosis, nuclear atypia, and expansion of the basal epithelium. Selective staining of lesions with at least one of three papillomavirus antibodies was observed in all cases (20 of 20). In contrast, immunostaining of lesions was negative for Epstein-Barr–related virus proteins (0 of 20). The unique similarities between the observed lesions and those seen in women suggest that macaques may provide a suitable animal model for study of papillomavirus oncogenesis.
Key words: Cervical intraepithelial neoplasia; immunohistochemistry; Macaca fascicularis; nonhuman primates; papillomavirus.
Request reprints from Dr. C. E. Wood, Comparative Medicine Clinical Research Center, Wake Forest University Health Sciences, Medical Center Boulevard, Winston-Salem, NC 27157-1040 (USA). E-mail: chwood@wfubmc.edu .
