

Is Cancer Contagious?
By David Holland, MD
I recently spoke with a nurse who was diagnosed, as an adult, with leukemia. She endured the chemotherapy regimen her doctors prescribed, only to suffer from a secondary fungal infection during that time. The intensity and duration of the antifungal treatment rivaled that of the chemotherapy. At any rate, she recovered from both afflictions and went back to work.
Later, as a result of another workup -- which included a liver biopsy -- for some returning symptoms she had, bad news was again brought up. "Your leukemia has returned," her oncologist told her, and he proceeded to lay out the next line of chemotherapy drugs she would have to take. Given that her chances of dying were much higher now that her cancer had returned, she opted to get a second opinion on her biopsy before proceeding with her next round of chemotherapy. She took her tissue sample to another hospital, and what she was told there was absolutely stunning: "You don't have leukemia," remarked the pathologist, "what you have is a fungal infection!"
The scenario that her doctors figured was that her previous fungal infection had returned -- a total possibility. But for this nurse, more questions were raised. She thought, for example, "If they diagnosed my fungal infection as leukemia this time, is it possible that they were wrong the FIRST time? Was my leukemia really a fungal infection to begin with, and was my so-called ´secondary´ fungal infection I had earlier really a full-blown manifestation of what originally might have looked like leukemia?"
Of course, she would never get answers to these questions, for to fully investigate thoughts like these might imply that a diagnostic error was made on the part of either her initial oncologist or pathologist. Nevertheless, an intense six months later -- some of it spent in the hospital -- of high-dose, powerful antifungals finally achieved a cure for her fungal infection. Today, she is again back at work, exuding more than ever with compassion for her patients. It really struck me when she told me where she works, because in her case, her occupation may very well relate to what she had suffered over the past two years. It turns out that she works at a bone-marrow transplant center, and is in daily contact with children with leukemia.
Now, the thought of her "acquiring" something as grave as leukemia would almost be preposterous to some. But the temptation to scratch our heads and wonder about this is unbearable. What if she really did have a fungal infection -- and NOT leukemia -- her first time around? And if so, did she "catch" this from her precious little patients?
Fungal infections not only can be extremely contagious, but they also go hand in hand with leukemia -- every oncologist knows this. And these infections are devastating: once a child who has become a bone marrow transplant recipient gets a "secondary" fungal infection, his chances of living, despite all the antifungals in the world, are only 20%, at best. And then the unthinkable thought arises: what if all of these children didn't even have leukemia, but rather a fungal infection, just as this nurse did? If doctors, in the 21st century, could mistake a fungal infection for leukemia in this nurse, could the same fate have fallen upon these children?
Doctors in general are not very good at diagnosing fungal infections because their medical school training is based so heavily on the role of bacteria and viruses in the area of infectious diseases. Fungi have been a forgotten foe ever since the advent of antibiotics. Once we had a drug that could kill bacteria, the interest in and the study of fungi fell to the wayside. Laboratories display the same difficulty in diagnosing fungal infections: current tests for detecting the presence of fungi are both terribly scant and sorely antiquated.
Despite these training and technical inadequacies, there have been at least a few good reports that implicate the role of fungi in causing leukemia. For example, in 1999 Meinolf Karthaus, MD, watched three different children with leukemia suddenly go into remission upon receiving a triple antifungal drug cocktail for their "secondary" fungal infections.(1) Pre-dating that, Marc Bielski stated back in 1997 that leukemia, whether acute or chronic, is intimately associated with the yeast, Candida albicans. (2) Finally, almost 50 years ago, Dr. J. Walter Wilson, in his textbook of clinical mycology, said that "it has been established that histoplasmosis and such reticuloendothelioses as leukemia, Hodgkin´s disease, lymphosarcoma, and sarcoidosis are found to be coexistent much more frequently than is statistically justifiable on the basis of coincidence." (3)
Histoplasmosis is what we call an "endemic" fungal infection. It is most commonly acquired in regions surrounding the Ohio and Mississippi river valleys in the United States. One becomes ill by merely inhaling the tiny fungal spores of this fungus. (For more information on histoplasmosis and other endemic fungi, you can visit: http://www.doctorfungus.org/). Three similar reports like this over the span of 40 years should convince us to at least study the role of fungi in cancers like leukemia a little more thoroughly.
The late Milton White, MD., did exactly this. He fully believed that cancer is a "chronic, intracellular, infectious, biologically induced spore (fungus) transformation disease." (4) Using the proper isolation techniques (involving saline instead of formaldehyde as a tissue transportation medium between the operating room and the pathology lab), he was able to find fungal spores in every sample of cancer tissue he studied. His lifetime work has been routinely dismissed as nothing more than an unproven postulate.
Regardless, wouldn´t you expect all of this information to make front-page headlines in every newspaper across the country, if not the world? Instead, every one of these findings was merely a brief mention -- only curious thoughts that one might entertain but never take seriously. The fact is, if leukemia and fungal infections "co-exist" so frequently, and if an antifungal drug cocktail effectively cured at least these three children of their leukemia, then I say we put the brakes on right there. Is there a need to go any farther, except to more deeply investigate the need for antifungals in treating leukemia and not just the secondary infections that arise in the course of chemotherapy?
In his book, The Germ that Causes Cancer (http://iknowthecause.com), author and television host Doug Kaufmann asserts that not only fungi, but also foods play a role in the etiology of cancer. He has seen children become free of their documented leukemia once the child´s parents simply changed the child´s diet. Kaufmann´s diet is base on the widely-published problem of mycotoxin contamination of our grain foods.
Grains such as corn, wheat, barley, sorghum, and other foods such as peanuts, are commonly contaminated with cancer-causing fungal poisons, or "mycotoxins." (5,6) One of them, called aflatoxin, just happens to be the most carcinogenic substance on earth. If this is indeed a problem, Kaufmann asserts, then cereal for breakfast and soda pop for dinner may not be conducive to a cancer-free lifestyle.
A case in point: in a grain-based diet, we consume, on average, from 0.15mg to 0.5mg of aflatoxin per day. (7) Further, he states, it is not the sugar alone that is the problem in our western diet, but the fungal toxins that are found in the sugary grains. More than once has Kaufmann interviewed a caller (on his health talk show) who absolutely craved peanut butter and popcorn just prior to their diagnosis of cancer.
Fungi are such a nuisance in carbohydrate foods in particular because fungi need carbohydrates to thrive. Therefore, it is rarer to see fungal contamination problems in foods like vegetables and high-protein foods. Kaufmann goes on further to explain how even antibiotics may play a role in the disease process. Antibiotics destroy the normal, protective gut bacteria, allowing intestinal yeast and fungi to grow unchecked. These internal, gut yeast make toxins, too. This can lead to immune suppression, symptoms of any autoimmune disease, or even cancer. "If the onset of any symptom or disease- cancer included- was preceded by a course of antibiotics," he maintains, "then look for a fungus to be at the root of your problem."
Doug and I will be talking more about the role of fungi in cancer and other diseases, such as diabetes, in our upcoming seminars. Check out our website (http://iknowthecause.com) to find the location nearest you.
David Holland, MD
Co-author, The Fungus Link, Infectious Diabetes.
20 May 2003
MediaTrition, Inc.
New research shows how vaccines cause immune system blood cells to divide into non-identical daughter cells. The researchers suspect that this may explain how blood cells can become cancerous, causing leukemia.
Researchers at the University of Pennsylvania’s Perelman School of Medicine have found how B lymphocytes produce non-identical daughter cells as part of the process of producing antibodies. Their paper on the study, “Asymmetric B Cell Division in the Germinal Center Reaction“, notes that:
Lifelong antibody responses to vaccination require reorganization of lymphoid tissue and dynamic inter-cellular communication called the germinal center reaction.
That is, the production of antibodies via vaccination changes the nature of lymph and the manner in which cells communicate. This is a significant, and serious, permanent change in the way the immune system functions. The authors themselves conclude this many explain how blood cells can turn become cancerous.
Unfortunately, the researchers don’t see, or don’t admit to seeing, the true implication:
Vaccines may be causing leukemia.
Instead, they see their discovery as an opportunity to find better vaccines! That’s rapidly becoming a primary source of income for Big Pharma, so it’s becoming a common statement in basic research. If a researcher hopes to continue receiving funds for studies, then it’s necessary to indicate that what they’ve found could be helpful in the mad dash after anything that might lead to more vaccines.
Antibody ProductionMacrophage is a term that comes from the Greek for “big eater”. Macrophage cells search and eat invaders, such as bacteria. Proteins from the eaten bacteria are broken down into their component peptides. These peptides are then attached to the surface of the macrophage.
When a T lymphocyte (commonly referred to as T-cells, which are so critical to AIDS patients) senses the same peptide on a B-cell that’s on a macrophage, it stimulates the B-cell to start producing antibodies.
The antibodies bind to the invaders, which makes it easier for white cells to ingest them. In some cases, the antibodies combine with an element of blood plasma, making them capable of killing the invaders outright.
The Difference Between Natural and Vaccine-Induced Immunity
We’re routinely told that our immune systems cannot tell the difference between natural and weakened invaders, or copies of bits of them that are commonly used in vaccines today. This, though, is far from from reality. The truth is that antigens are not readily formed from these weakened and partial pathogens, which clearly indicates that macrophages do see the difference between genuine invaders and injected pseudo-invaders.
That’s why adjuvants are used. They stimulate the macrophages to trigger the production of antibodies. What exactly are the macrophages responding to? That is unknown. What sort of peptides are they attaching to the surface of their cells? Why should we believe that these peptides are exactly the same as those produced when macrophages respond to genuine invasions?
Finally, we need to ask what these pseudo-pathogens, combined with adjuvants, are doing to the macrophages. Are they producing mutated cells? We do not know.
The ResearchThe study investigated how antibodies are made after vaccination. It has long been known to happen in a manner different from natural immunity.
Production of Daughter Cells by B-cells
As noted above, B-cells produced by macrophages in turn produce antibodies when stimulated by T-cells. The new research investigated this process. When stimulated, B-cells divide. However, unlike typical cell division, in which two identical daughter cells are produced, B-cells split into two different kinds of cells.
One of the daughter cells contains three types of proteins that determine what kinds of antibodies to produce, and these B-cells divide into replicas of themselves. The other type of daughter cell apparently improves the quality of the antibodies produced.
By David Holland, MD
I recently spoke with a nurse who was diagnosed, as an adult, with leukemia. She endured the chemotherapy regimen her doctors prescribed, only to suffer from a secondary fungal infection during that time. The intensity and duration of the antifungal treatment rivaled that of the chemotherapy. At any rate, she recovered from both afflictions and went back to work.
Later, as a result of another workup -- which included a liver biopsy -- for some returning symptoms she had, bad news was again brought up. "Your leukemia has returned," her oncologist told her, and he proceeded to lay out the next line of chemotherapy drugs she would have to take. Given that her chances of dying were much higher now that her cancer had returned, she opted to get a second opinion on her biopsy before proceeding with her next round of chemotherapy. She took her tissue sample to another hospital, and what she was told there was absolutely stunning: "You don't have leukemia," remarked the pathologist, "what you have is a fungal infection!"
The scenario that her doctors figured was that her previous fungal infection had returned -- a total possibility. But for this nurse, more questions were raised. She thought, for example, "If they diagnosed my fungal infection as leukemia this time, is it possible that they were wrong the FIRST time? Was my leukemia really a fungal infection to begin with, and was my so-called ´secondary´ fungal infection I had earlier really a full-blown manifestation of what originally might have looked like leukemia?"
Of course, she would never get answers to these questions, for to fully investigate thoughts like these might imply that a diagnostic error was made on the part of either her initial oncologist or pathologist. Nevertheless, an intense six months later -- some of it spent in the hospital -- of high-dose, powerful antifungals finally achieved a cure for her fungal infection. Today, she is again back at work, exuding more than ever with compassion for her patients. It really struck me when she told me where she works, because in her case, her occupation may very well relate to what she had suffered over the past two years. It turns out that she works at a bone-marrow transplant center, and is in daily contact with children with leukemia.
Now, the thought of her "acquiring" something as grave as leukemia would almost be preposterous to some. But the temptation to scratch our heads and wonder about this is unbearable. What if she really did have a fungal infection -- and NOT leukemia -- her first time around? And if so, did she "catch" this from her precious little patients?
Fungal infections not only can be extremely contagious, but they also go hand in hand with leukemia -- every oncologist knows this. And these infections are devastating: once a child who has become a bone marrow transplant recipient gets a "secondary" fungal infection, his chances of living, despite all the antifungals in the world, are only 20%, at best. And then the unthinkable thought arises: what if all of these children didn't even have leukemia, but rather a fungal infection, just as this nurse did? If doctors, in the 21st century, could mistake a fungal infection for leukemia in this nurse, could the same fate have fallen upon these children?
Doctors in general are not very good at diagnosing fungal infections because their medical school training is based so heavily on the role of bacteria and viruses in the area of infectious diseases. Fungi have been a forgotten foe ever since the advent of antibiotics. Once we had a drug that could kill bacteria, the interest in and the study of fungi fell to the wayside. Laboratories display the same difficulty in diagnosing fungal infections: current tests for detecting the presence of fungi are both terribly scant and sorely antiquated.
Despite these training and technical inadequacies, there have been at least a few good reports that implicate the role of fungi in causing leukemia. For example, in 1999 Meinolf Karthaus, MD, watched three different children with leukemia suddenly go into remission upon receiving a triple antifungal drug cocktail for their "secondary" fungal infections.(1) Pre-dating that, Marc Bielski stated back in 1997 that leukemia, whether acute or chronic, is intimately associated with the yeast, Candida albicans. (2) Finally, almost 50 years ago, Dr. J. Walter Wilson, in his textbook of clinical mycology, said that "it has been established that histoplasmosis and such reticuloendothelioses as leukemia, Hodgkin´s disease, lymphosarcoma, and sarcoidosis are found to be coexistent much more frequently than is statistically justifiable on the basis of coincidence." (3)
Histoplasmosis is what we call an "endemic" fungal infection. It is most commonly acquired in regions surrounding the Ohio and Mississippi river valleys in the United States. One becomes ill by merely inhaling the tiny fungal spores of this fungus. (For more information on histoplasmosis and other endemic fungi, you can visit: http://www.doctorfungus.org/). Three similar reports like this over the span of 40 years should convince us to at least study the role of fungi in cancers like leukemia a little more thoroughly.
The late Milton White, MD., did exactly this. He fully believed that cancer is a "chronic, intracellular, infectious, biologically induced spore (fungus) transformation disease." (4) Using the proper isolation techniques (involving saline instead of formaldehyde as a tissue transportation medium between the operating room and the pathology lab), he was able to find fungal spores in every sample of cancer tissue he studied. His lifetime work has been routinely dismissed as nothing more than an unproven postulate.
Regardless, wouldn´t you expect all of this information to make front-page headlines in every newspaper across the country, if not the world? Instead, every one of these findings was merely a brief mention -- only curious thoughts that one might entertain but never take seriously. The fact is, if leukemia and fungal infections "co-exist" so frequently, and if an antifungal drug cocktail effectively cured at least these three children of their leukemia, then I say we put the brakes on right there. Is there a need to go any farther, except to more deeply investigate the need for antifungals in treating leukemia and not just the secondary infections that arise in the course of chemotherapy?
In his book, The Germ that Causes Cancer (http://iknowthecause.com), author and television host Doug Kaufmann asserts that not only fungi, but also foods play a role in the etiology of cancer. He has seen children become free of their documented leukemia once the child´s parents simply changed the child´s diet. Kaufmann´s diet is base on the widely-published problem of mycotoxin contamination of our grain foods.
Grains such as corn, wheat, barley, sorghum, and other foods such as peanuts, are commonly contaminated with cancer-causing fungal poisons, or "mycotoxins." (5,6) One of them, called aflatoxin, just happens to be the most carcinogenic substance on earth. If this is indeed a problem, Kaufmann asserts, then cereal for breakfast and soda pop for dinner may not be conducive to a cancer-free lifestyle.
A case in point: in a grain-based diet, we consume, on average, from 0.15mg to 0.5mg of aflatoxin per day. (7) Further, he states, it is not the sugar alone that is the problem in our western diet, but the fungal toxins that are found in the sugary grains. More than once has Kaufmann interviewed a caller (on his health talk show) who absolutely craved peanut butter and popcorn just prior to their diagnosis of cancer.
Fungi are such a nuisance in carbohydrate foods in particular because fungi need carbohydrates to thrive. Therefore, it is rarer to see fungal contamination problems in foods like vegetables and high-protein foods. Kaufmann goes on further to explain how even antibiotics may play a role in the disease process. Antibiotics destroy the normal, protective gut bacteria, allowing intestinal yeast and fungi to grow unchecked. These internal, gut yeast make toxins, too. This can lead to immune suppression, symptoms of any autoimmune disease, or even cancer. "If the onset of any symptom or disease- cancer included- was preceded by a course of antibiotics," he maintains, "then look for a fungus to be at the root of your problem."
Doug and I will be talking more about the role of fungi in cancer and other diseases, such as diabetes, in our upcoming seminars. Check out our website (http://iknowthecause.com) to find the location nearest you.
David Holland, MD
Co-author, The Fungus Link, Infectious Diabetes.
20 May 2003
MediaTrition, Inc.
New research shows how vaccines cause immune system blood cells to divide into non-identical daughter cells. The researchers suspect that this may explain how blood cells can become cancerous, causing leukemia.
Researchers at the University of Pennsylvania’s Perelman School of Medicine have found how B lymphocytes produce non-identical daughter cells as part of the process of producing antibodies. Their paper on the study, “Asymmetric B Cell Division in the Germinal Center Reaction“, notes that:
Lifelong antibody responses to vaccination require reorganization of lymphoid tissue and dynamic inter-cellular communication called the germinal center reaction.
That is, the production of antibodies via vaccination changes the nature of lymph and the manner in which cells communicate. This is a significant, and serious, permanent change in the way the immune system functions. The authors themselves conclude this many explain how blood cells can turn become cancerous.
Unfortunately, the researchers don’t see, or don’t admit to seeing, the true implication:
Vaccines may be causing leukemia.
Instead, they see their discovery as an opportunity to find better vaccines! That’s rapidly becoming a primary source of income for Big Pharma, so it’s becoming a common statement in basic research. If a researcher hopes to continue receiving funds for studies, then it’s necessary to indicate that what they’ve found could be helpful in the mad dash after anything that might lead to more vaccines.
Antibody ProductionMacrophage is a term that comes from the Greek for “big eater”. Macrophage cells search and eat invaders, such as bacteria. Proteins from the eaten bacteria are broken down into their component peptides. These peptides are then attached to the surface of the macrophage.
When a T lymphocyte (commonly referred to as T-cells, which are so critical to AIDS patients) senses the same peptide on a B-cell that’s on a macrophage, it stimulates the B-cell to start producing antibodies.
The antibodies bind to the invaders, which makes it easier for white cells to ingest them. In some cases, the antibodies combine with an element of blood plasma, making them capable of killing the invaders outright.
The Difference Between Natural and Vaccine-Induced Immunity
We’re routinely told that our immune systems cannot tell the difference between natural and weakened invaders, or copies of bits of them that are commonly used in vaccines today. This, though, is far from from reality. The truth is that antigens are not readily formed from these weakened and partial pathogens, which clearly indicates that macrophages do see the difference between genuine invaders and injected pseudo-invaders.
That’s why adjuvants are used. They stimulate the macrophages to trigger the production of antibodies. What exactly are the macrophages responding to? That is unknown. What sort of peptides are they attaching to the surface of their cells? Why should we believe that these peptides are exactly the same as those produced when macrophages respond to genuine invasions?
Finally, we need to ask what these pseudo-pathogens, combined with adjuvants, are doing to the macrophages. Are they producing mutated cells? We do not know.
The ResearchThe study investigated how antibodies are made after vaccination. It has long been known to happen in a manner different from natural immunity.
Production of Daughter Cells by B-cells
As noted above, B-cells produced by macrophages in turn produce antibodies when stimulated by T-cells. The new research investigated this process. When stimulated, B-cells divide. However, unlike typical cell division, in which two identical daughter cells are produced, B-cells split into two different kinds of cells.
One of the daughter cells contains three types of proteins that determine what kinds of antibodies to produce, and these B-cells divide into replicas of themselves. The other type of daughter cell apparently improves the quality of the antibodies produced.
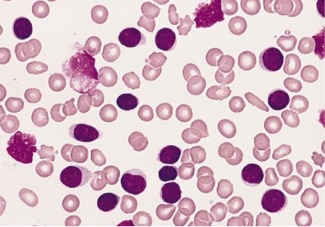
Blood smear of lymphocytosis in B-Cell leukemia. The light colored cells are lymphocytes. You can readily see three severely damaged cancerous cells. (Photo is public domain, from the Armed Forces Institute of Pathology in the US, PEIR Digital Laboratory.)
This brings into question the nature of the cells that result from vaccine-induced peptides on macrophages. Do they truly match those of genuine invaders? Could they result in the production of defective B-cells, even ones that are cancerous? B-cells are a type of white blood cell, and there is a type of leukemia, as noted in the graphic to the left, called B-cell lymphoma.
If any possible association between an increase in vaccinations and an increase in leukemia can be shown, then caution should certainly indicate that the potential of vaccine-induced leukemia should be investigated. As it turns out, such an association can be readily demonstrated.
This brings into question the nature of the cells that result from vaccine-induced peptides on macrophages. Do they truly match those of genuine invaders? Could they result in the production of defective B-cells, even ones that are cancerous? B-cells are a type of white blood cell, and there is a type of leukemia, as noted in the graphic to the left, called B-cell lymphoma.
If any possible association between an increase in vaccinations and an increase in leukemia can be shown, then caution should certainly indicate that the potential of vaccine-induced leukemia should be investigated. As it turns out, such an association can be readily demonstrated.
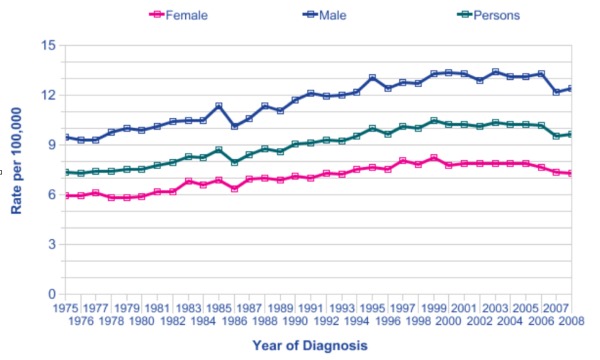
Leukaemia European Age-Standardised Incidence Rates, Great Britain, 1975-2008 (Graph from Cancer Research UK)
This graph from Cancer Research UK provides a clear association between increased vaccination rates in Great Britain and increased leukemia rates. Though the incidence of diagnosed leukemia has decreased recently, it can’t, at this point, be indicative of a trend. As can be seen on the graph, such temporary decreases have occurred before without affecting the general trend.
It should be noted that acute lymphocytic leukemia (ALL), a B-cell type, is most commonly diagnosed in children. 63.6% of all such cases are diagnosed in people under age 20 years. Since B-cells are significant in vaccine-produced immunity, could the increase in ALL be a significant part of the increase in leukemia? As it turns out, the answer is yes. From 1982-2001, the incidence rate of B-precursor ALL in nordic countries increased from 2.92 to 3.59 per 100,000--an increase of 23 percent in children.
A correlation between an increase in B-cell related leukemia in children and the increased rate of vaccinations does exist. So, we have both a correlation in a leukemia that’s related to B-cells and leukemia in general. Plus, this study demonstrates that the mechanism of vaccine-derived antibodies utilizes B-cells.
It is, therefore, reasonable to suggest that there may be a causal link between vaccinations and leukemia. Certainly, the evidence such a potential indicates that, rather than investigating yet more types of vaccines, medical science should be devoting itself to investigating the risk of vaccine-induced leukemia.
Deranged Immune SystemNot only is leukemia now an implied risk of vaccinations, as discussed in other Gaia Health articles, a downward trend in children’s health may also be a result of vaccine damage. This study shows the potential of deranged immune systems resulting from vaccinations. We can also see that disease immunity produced by vaccines, if any exists at all, is likely defective.
We are seeing massive increases in chronic diseases, especially in children—Autism. Cancer. Allergies. Asthma. Diabetes. Neurological Disorders. It begs credulity to suggest that there’s been a major shift in genetics causing it. Clearly, it’s time to face this reality and stop sending good money after bad. Research needs to focus on causes for which we have evidence of a connection. There can be little question that the rise of these chronic disorders in children—not to mention many in adults, such as Alzheimer’s disease—exist in a trajectory similar to the rise in vaccinations.
With the health and well-being of virtually all humanity now apparently at risk, it’s long past time to face this issue. We must demand honest research in causes of all this ill health, with a focus on a likely connection with vaccinations.
With great appreciation to Jagannath Chatterjee
for bringing this research to my attention.
Resources: Asymmetric B Cell Division in the Germinal Center ReactionHow B Cells May Generate Antibodies After VaccinationPenn Study Shows How B Cells May Generate Antibodies After VaccinationHow Lymphcytes Produce AntibodyLeukaemia – UK Incidence StatisticsAge- and Sex-Specific Incidence of Childhood Leukemia by Immunophenotype in the Nordic CountriesAcute Lymphocytic Leukemia Statistic
This graph from Cancer Research UK provides a clear association between increased vaccination rates in Great Britain and increased leukemia rates. Though the incidence of diagnosed leukemia has decreased recently, it can’t, at this point, be indicative of a trend. As can be seen on the graph, such temporary decreases have occurred before without affecting the general trend.
It should be noted that acute lymphocytic leukemia (ALL), a B-cell type, is most commonly diagnosed in children. 63.6% of all such cases are diagnosed in people under age 20 years. Since B-cells are significant in vaccine-produced immunity, could the increase in ALL be a significant part of the increase in leukemia? As it turns out, the answer is yes. From 1982-2001, the incidence rate of B-precursor ALL in nordic countries increased from 2.92 to 3.59 per 100,000--an increase of 23 percent in children.
A correlation between an increase in B-cell related leukemia in children and the increased rate of vaccinations does exist. So, we have both a correlation in a leukemia that’s related to B-cells and leukemia in general. Plus, this study demonstrates that the mechanism of vaccine-derived antibodies utilizes B-cells.
It is, therefore, reasonable to suggest that there may be a causal link between vaccinations and leukemia. Certainly, the evidence such a potential indicates that, rather than investigating yet more types of vaccines, medical science should be devoting itself to investigating the risk of vaccine-induced leukemia.
Deranged Immune SystemNot only is leukemia now an implied risk of vaccinations, as discussed in other Gaia Health articles, a downward trend in children’s health may also be a result of vaccine damage. This study shows the potential of deranged immune systems resulting from vaccinations. We can also see that disease immunity produced by vaccines, if any exists at all, is likely defective.
We are seeing massive increases in chronic diseases, especially in children—Autism. Cancer. Allergies. Asthma. Diabetes. Neurological Disorders. It begs credulity to suggest that there’s been a major shift in genetics causing it. Clearly, it’s time to face this reality and stop sending good money after bad. Research needs to focus on causes for which we have evidence of a connection. There can be little question that the rise of these chronic disorders in children—not to mention many in adults, such as Alzheimer’s disease—exist in a trajectory similar to the rise in vaccinations.
With the health and well-being of virtually all humanity now apparently at risk, it’s long past time to face this issue. We must demand honest research in causes of all this ill health, with a focus on a likely connection with vaccinations.
With great appreciation to Jagannath Chatterjee
for bringing this research to my attention.
Resources: Asymmetric B Cell Division in the Germinal Center ReactionHow B Cells May Generate Antibodies After VaccinationPenn Study Shows How B Cells May Generate Antibodies After VaccinationHow Lymphcytes Produce AntibodyLeukaemia – UK Incidence StatisticsAge- and Sex-Specific Incidence of Childhood Leukemia by Immunophenotype in the Nordic CountriesAcute Lymphocytic Leukemia Statistic
